

Infection prevention and control risk factors for SARS-CoV-2 infection in health workers: a global, multi-centre, case-control study
- PMID: 39307426
- PMCID: PMC11748119
- DOI: 10.1016/j.jhin.2024.04.031
Infection prevention and control risk factors for SARS-CoV-2 infection in health workers: a global, multi-centre, case-control study
Abstract
Background: Health workers were at higher risk for severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection during the coronavirus disease 2019 (COVID-19) pandemic due to occupational risk factors. This study aimed to characterize these risk factors as part of the World Health Organization (WHO) Unity Studies initiative.
Methods: This global, multi-centre, nested, case-control study was conducted in 121 healthcare facilities in 21 countries. Cases were health workers who tested positive for SARS-CoV-2 infection with documented occupational exposure to COVID-19 patients in the 14 days pre-enrolment. Controls were enrolled from the same facilities with similar exposure but negative serology. Case and control status was confirmed with serological testing at baseline and after 3-4 weeks. Demographic and infection risk factor data were collected using structured questionnaires.
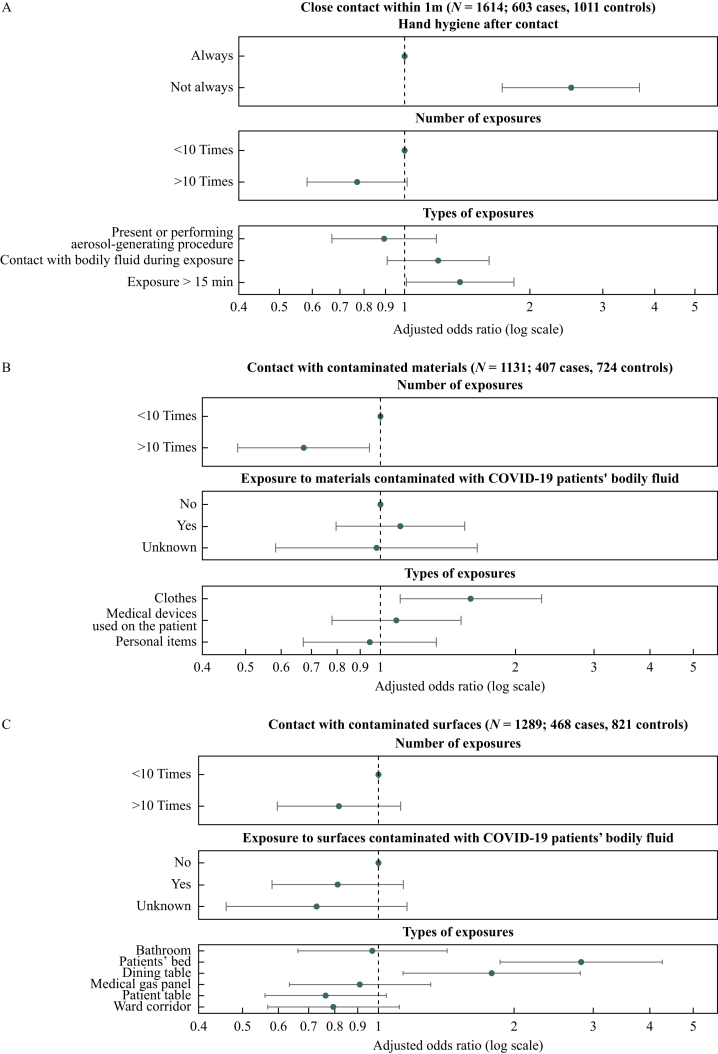
Findings: Between June 2020 and December 2021, data were obtained for 1213 cases and 1844 controls. Risk of SARS-CoV-2 infection was associated with non-adherence to personal protective equipment (PPE) guidelines [adjusted odds ratio (aOR) 1.67, 95% confidence interval (CI) 1.32-2.12] and not performing hand hygiene consistently after patient contact (aOR 2.52, 95% CI 1.72-3.68). Direct close contact with COVID-19 patients was also associated with increased risk of SARS-CoV-2 infection, particularly during prolonged contact (>15 min). Items associated with lower risk of SARS-CoV-2 infection were use of a respirator during aerosol-generating procedures; and use of gloves, and a gown or coverall during contact with contaminated materials/surfaces. No difference was observed between health workers using respirators vs surgical masks for routine care.
Conclusion: Appropriate implementation of infection prevention and control measures and use of PPE remain a priority to protect health workers from SARS-CoV-2 infection.
Keywords: Adherence; COVID-19; Health workers; Infection prevention and control; Occupational risk factors; Personal protective equipment; SARS-CoV-2.
Copyright © 2024. Published by Elsevier Ltd.
Conflict of interest statement
Conflict of interest statement None declared.
Figures


References
-
- World Health Organization . WHO; Geneva: 2021. The impact of COVID-19 on health and care workers: a closer look at deaths.https://apps.who.int/iris/handle/10665/345300 Available at:
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
