

Modified Bridge-Enhanced Anterior Cruciate Ligament Repair
- PMID: 39308585
- PMCID: PMC11411291
- DOI: 10.1016/j.eats.2024.103034
Modified Bridge-Enhanced Anterior Cruciate Ligament Repair
Abstract
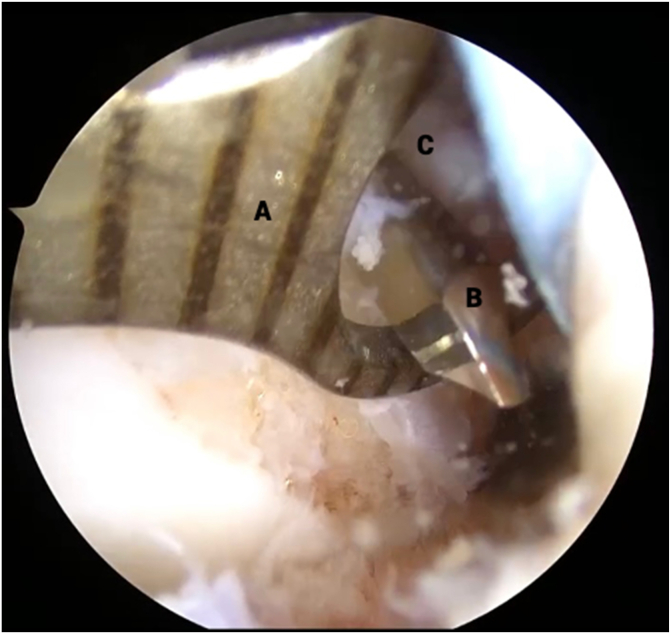
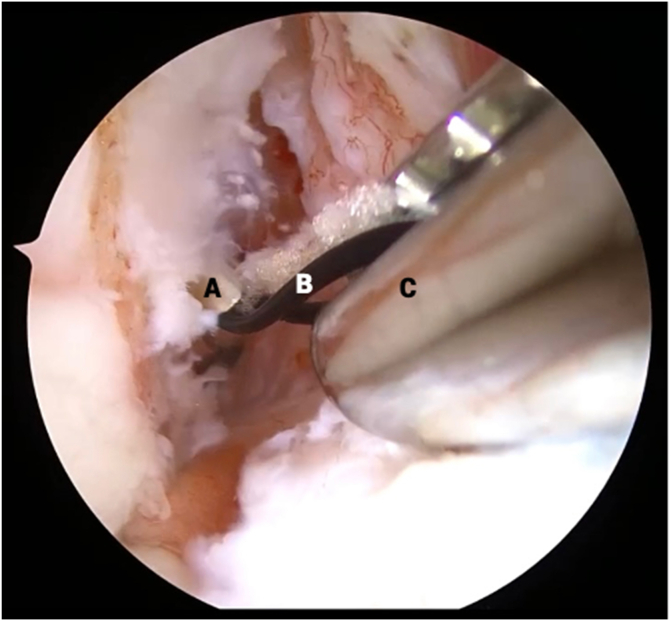
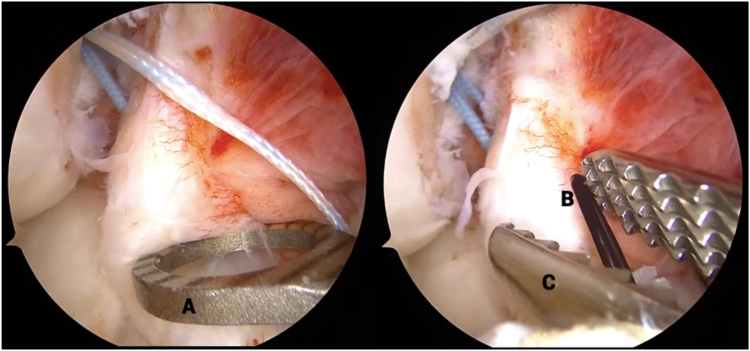
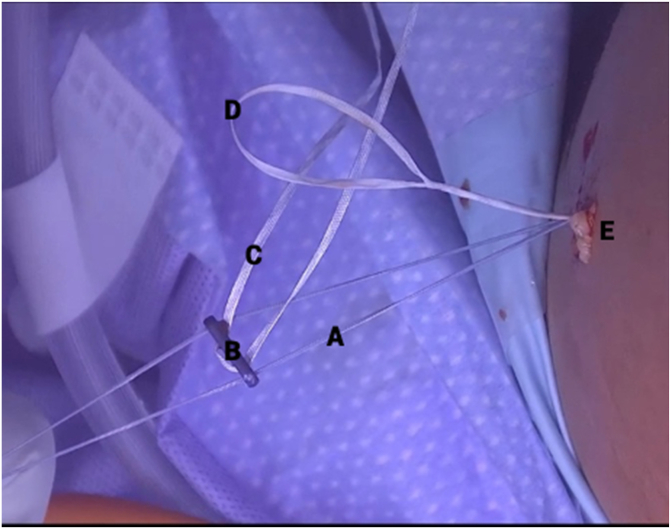
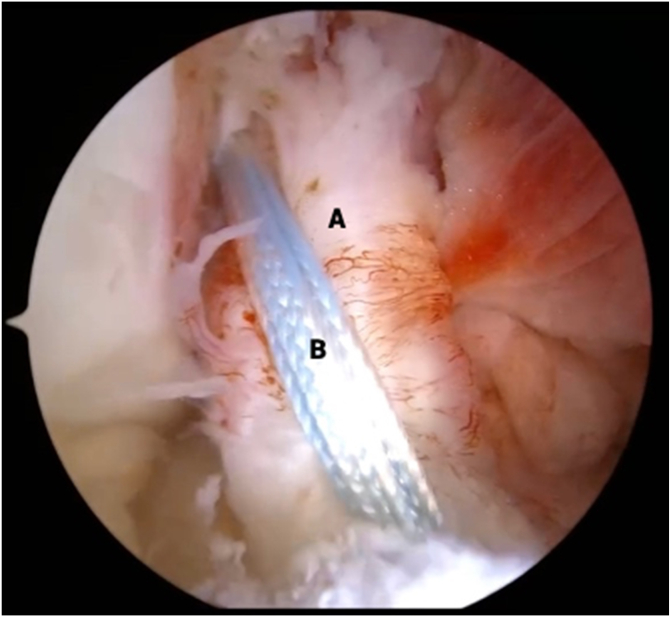
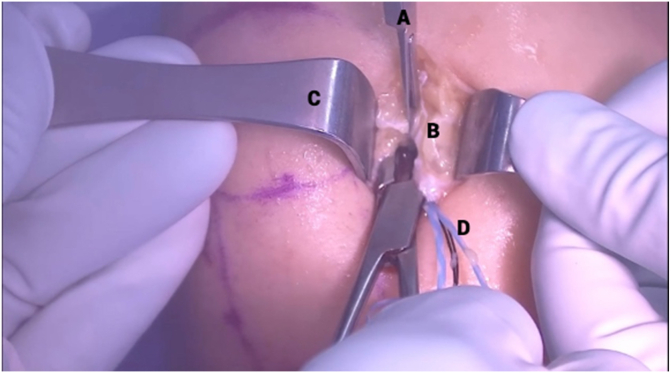
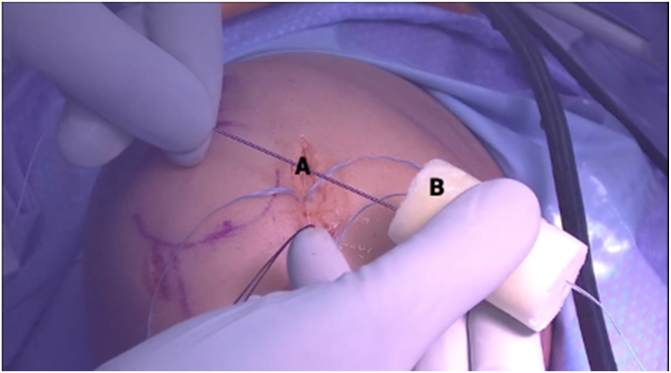
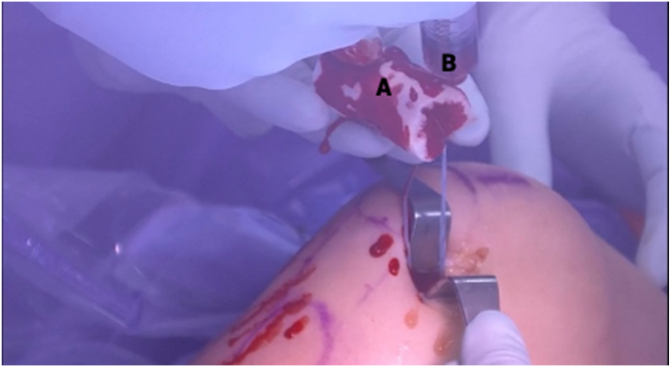
Historically, the treatment of anterior cruciate ligament (ACL) injuries shifted from primary repair to reconstruction because the native, intrasynovial location of the ACL precluded the formation of a fibrin-rich clot needed for ligament healing. However, increasing attention has been paid to augmenting the biological environment surrounding the ACL to facilitate its healing after arthroscopic repair. The bridge-enhanced ACL restoration implant uses resorbable collagen mixed with autologous blood to provide a biological scaffold for tissue healing. The short-term results of this procedure are promising, showing noninferiority to traditional ACL reconstruction at 2 years postoperatively and a higher rate of return to sport at 6 months. Our technique for performing the bridge-enhanced ACL repair is efficient, is easy to learn, and achieves excellent fixation of the ACL stump augmented with an internal brace.
© 2024 The Authors.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: J.N.G. reports a consulting or advisory relationship with DePuy Synthes Mitek Sports Medicine. S.G.A. reports a consulting or advisory relationship with Miach Orthopaedics. All other authors (D.E.K., C.N.D., E.D.H.) declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures


References
-
- Sanders T.L., Maradit Kremers H., Bryan A.J., et al. Incidence of anterior cruciate ligament tears and reconstruction: A 21-year population-based study. Am J Sports Med. 2016;44:1502–1507. - PubMed
-
- Feagin J.A., Curl W.W. Isolated tear of the anterior cruciate ligament: 5-Year follow-up study. Am J Sports Med. 1976;4:95–100. - PubMed
-
- Odensten M., Hamberg P., Nordin M., Lysholm J., Gillquist J. Surgical or conservative treatment of the acutely torn anterior cruciate ligament: A randomized study with short-term follow-up observations. Clin Orthop Relat Res. 1985;198:87–93. - PubMed
-
- Sandberg R., Balkfors B., Nilsson B., Westlin N. Operative versus non-operative treatment of recent injuries to the ligaments of the knee. A prospective randomized study. J Bone Joint Surg Am. 1987;69:1120–1126. - PubMed
LinkOut - more resources
Full Text Sources
