

532 nm versus 810 nm subthreshold micropulse laser in treatment of non-resolving central serous chorioretinopathy: A randomized controlled trial
- PMID: 39309578
- PMCID: PMC11411298
- DOI: 10.1016/j.mjafi.2022.12.011
532 nm versus 810 nm subthreshold micropulse laser in treatment of non-resolving central serous chorioretinopathy: A randomized controlled trial
Abstract
Background: The relative efficacy of 532 nm subthreshold micropulse laser in comparison to the 810 nm subthreshold micropulse laser, in the treatment of central serous chorioretinopathy is not known.
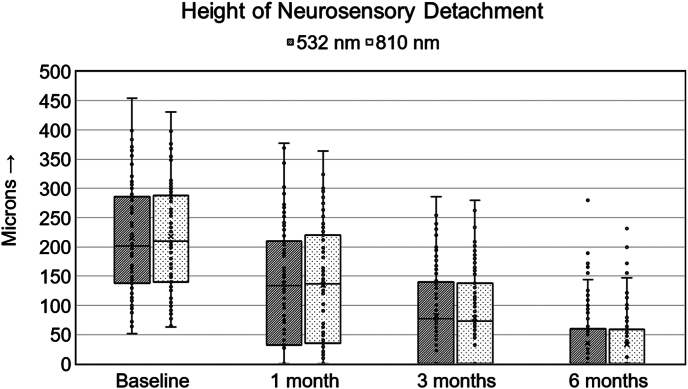
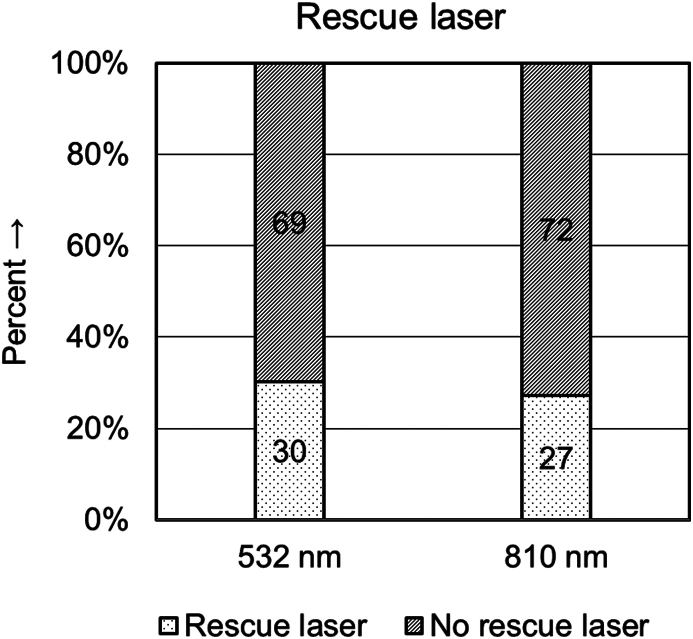
Methods: This randomized controlled trial included 99 eyes each in groups A and B. Key inclusion criteria were: (i) vision loss for minimum three months due to persistent central serous chorioretinopathy; (ii) focal leaks (upto two leaks) on fundus fluorescein angiography. Key exclusion criteria were: (i) history of prior treatment for central serous chorioretinopathy; (ii) absence of any leak/ presence of diffuse leaks/ >2 leaks on fundus fluorescein angiography; (iii) chronic central serous chorioretinopathy. All eyes were treated with subthreshold micropulse laser (group A: 532 nm green laser; group B: 810 nm diode laser). Best-corrected visual acuity, autofluorescence, spectral domain optical coherence tomography, and fundus fluorescein angiography, were evaluated at baseline and at 1, 3, and 6 months. Laser was repeated in nor-responders at 3 months.
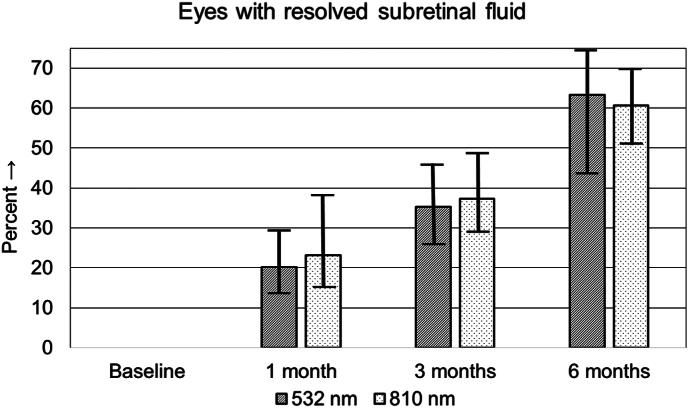
Results: There was a statistically significant improvement in BCVA in both groups six months post laser. Between the two groups, a comparable proportion of eyes showed complete resolution of subretinal fluid at one month, three months and at six months. No adverse effect of laser was observed in either group.
Conclusion: Both 532 nm STMP laser and 810 nm STMP laser have comparable structural and functional outcomes in the treatment of non-resolving CSC. There are no adverse effects related to either of the two wavelengths.
Keywords: Central serous chorioretinopathy; Sub-retinal fluid; Subthreshold micropulse laser.
© 2023 Director General, Armed Forces Medical Services. Published by Elsevier, a division of RELX India Pvt. Ltd.
Conflict of interest statement
The authors have none to declare.
Figures


References
-
- Ulbig M.R., Arden G.B., Hamilton A.P. Color contrast sensitivity and pattern electroretinographic findings after diode and argon laser photocoagulation in diabetic retinopathy. Am J Ophthalmol. 1994;117(5):583–588. - PubMed
-
- Lewen R.M. Subretinal neovascularization complicating laser photocoagulation of diabetic maculopathy. Ophthal Surg Lasers Imaging Retina. 1988;19(10):734–737. - PubMed
-
- Smith C.W., Guyer D.R., D'Amico D.J. Subretinal fibrosis after laser photocoagulation for diabetic macular edema. Am J Ophthalmol. 1992;113(6):652–656. - PubMed
-
- Seiberth V., Alexandridis E., Feng W. Function of the diabetic retina after panretinal argon laser coagulation. Graefes Arch Clin Exp Ophthalmol. 1987;225(6):385–390. - PubMed
-
- Pearson A., Tanner V., Keightley S., Casswell A. What effect does laser photocoagulation have on driving visual fields in diabetics? Eye (Lond). 1998;12(1):64–68. - PubMed
LinkOut - more resources
Full Text Sources
