

Relevance of plasma lipoproteins and small metabolites in assessment of nutritional status among patients with severe injuries
- PMID: 39310068
- PMCID: PMC11411433
- DOI: 10.1016/j.jointm.2024.02.004
Relevance of plasma lipoproteins and small metabolites in assessment of nutritional status among patients with severe injuries
Abstract
Background: This study aimed to identify plasma lipoproteins and small metabolites associated with high risk of malnutrition during intensive care unit (ICU) stay in patients with severe injuries.
Methods: This observational prospective exploratory study was conducted at two level-1 trauma centers in the Netherlands. Adult patients (aged ≥18 years) who were admitted to the ICU for more than 48 h between July 2018 and April 2022 owing to severe injuries (polytrauma, as defined by Injury Severity Scores of ≥16) caused by blunt trauma were eligible for inclusion. Partial least squares discriminant analysis was used to analyze the relationship of 112 lipoprotein-related components and 23 small metabolites with the risk of malnutrition (modified Nutrition Risk in Critically Ill score). Malnutrition was diagnosed based on Subjective Global Assessment scores. The relationship of lipoprotein properties and small metabolite concentrations with malnutrition (during ICU admission) was evaluated using mixed effects logistic regression.
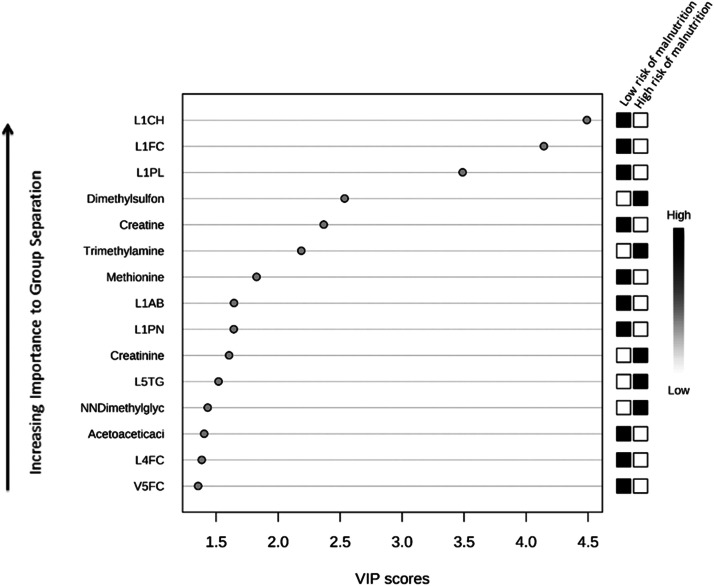
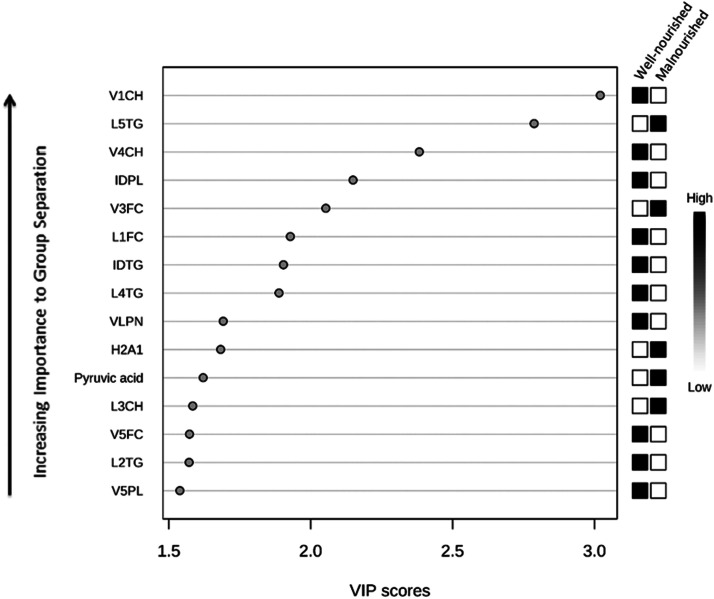
Results: Overall, 51 patients were included. Lower (very) low-density lipoprotein ([V]LDL) (free) cholesterol and phospholipid levels, low particle number, and higher levels of LDL triglycerides were associated with a higher risk of malnutrition (variable importance in projection [VIP] value >1.5). Low levels of most (V)LDL and intermediate-density lipoprotein subfractions and high levels of high-density lipoprotein Apo-A1 were associated with the diagnosis of malnutrition (VIP value >1.5). Increased levels of dimethyl sulfone, trimethylamine N-oxide, creatinine, N, N-dimethylglycine, and pyruvic acid and decreased levels of creatine, methionine, and acetoacetic acid were also indicative of malnutrition (VIP value >1.5). Overall, 14 lipoproteins and 1 small metabolite were significantly associated with a high risk of malnutrition during ICU admission (P <0.05); however, the association did not persist after correcting the false discovery rate (P=0.35 for all).
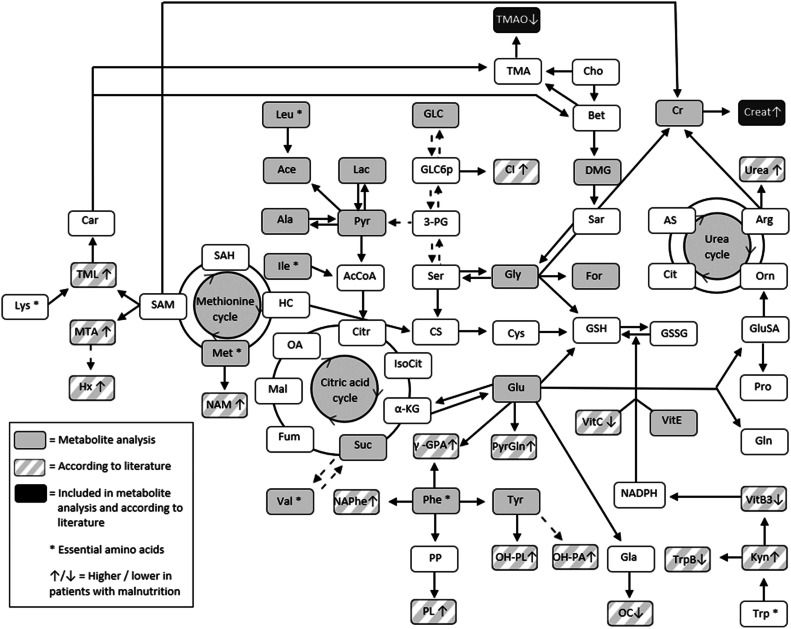
Conclusion: Increased triglyceride in several lipoprotein subfractions and decreased levels of other lipoprotein subfraction lipids and several small metabolites (involved in the homocysteine cycle, ketone body formation, and muscle metabolism) may be indicative of malnutrition risk. Following validation in larger cohorts, these indicators may guide institution of preventive nutritional measures in patients admitted to the ICU with severe injuries.
Keywords: Lipoproteins; Malnutrition; Metabolites; Nutritional status; Severely injured; Trauma.
© 2024 The Author(s).
Figures

Similar articles
-
Association of modified NUTRIC score for nutritional risk and in-hospital developed malnutrition in adults with severe injuries: a prospective observational cohort study.Eur J Trauma Emerg Surg. 2025 May 20;51(1):214. doi: 10.1007/s00068-025-02887-7. Eur J Trauma Emerg Surg. 2025. PMID: 40394257 Free PMC article.
-
The correlation of CT-derived muscle density, skeletal muscle index, and visceral adipose tissue with nutritional status in severely injured patients.Eur J Trauma Emerg Surg. 2024 Dec;50(6):3209-3215. doi: 10.1007/s00068-024-02624-6. Epub 2024 Aug 21. Eur J Trauma Emerg Surg. 2024. PMID: 39167212 Free PMC article.
-
The malnutrition in polytrauma patients (MaPP) study: Research protocol.Nutr Health. 2019 Dec;25(4):291-301. doi: 10.1177/0260106019868884. Epub 2019 Aug 28. Nutr Health. 2019. PMID: 31456469 Free PMC article.
-
Prevalence, incidence, and complications of malnutrition in severely injured patients.Eur J Trauma Emerg Surg. 2025 Jan 24;51(1):72. doi: 10.1007/s00068-024-02711-8. Eur J Trauma Emerg Surg. 2025. PMID: 39856269 Free PMC article.
-
Feeding the critically ill obese patient: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Oct;13(10):95-109. doi: 10.11124/jbisrir-2015-2458. JBI Database System Rev Implement Rep. 2015. PMID: 26571286
References
-
- Jensen G.L., Mirtallo J., Compher C., Dhaliwal R., Forbes A., Grijalba R.F., et al. Adult starvation and disease-related malnutrition: a proposal for etiology-based diagnosis in the clinical practice setting from the International Consensus Guideline Committee. JPEN J Parenter Enteral Nutr. 2010;34(2):156–159. doi: 10.1177/0148607110361910. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
