

Network Analysis of Pain Catastrophizing, Self-Efficacy, and Kinesiophobia Among Patients After Total Knee Arthroplasty: A Cross-Sectional Study
- PMID: 39310086
- PMCID: PMC11414755
- DOI: 10.2147/PPA.S452773
Network Analysis of Pain Catastrophizing, Self-Efficacy, and Kinesiophobia Among Patients After Total Knee Arthroplasty: A Cross-Sectional Study
Abstract
Background: Kinesiophobia is common in patients after total knee arthroplasty and is an important risk factor for post-operative recovery outcomes. Little is known about the complex intercorrelations between different components of pain catastrophizing, self-efficacy, and kinesiophobia. This study aimed to identify the central components of kinesiophobia and to explore the interconnectedness between components of pain catastrophizing, self-efficacy, and kinesiophobia.
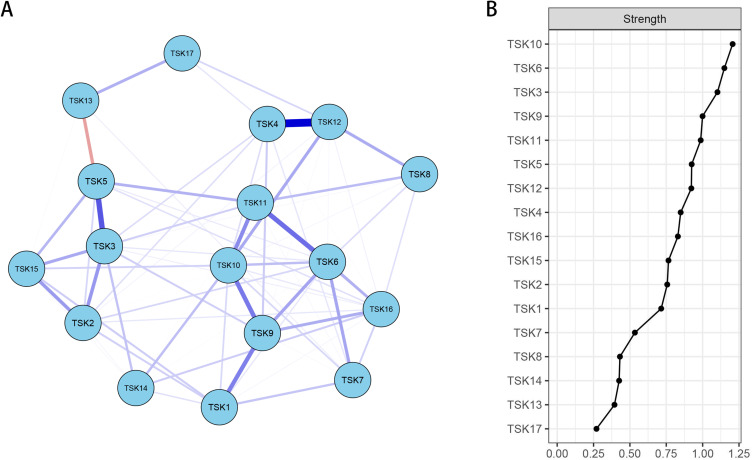
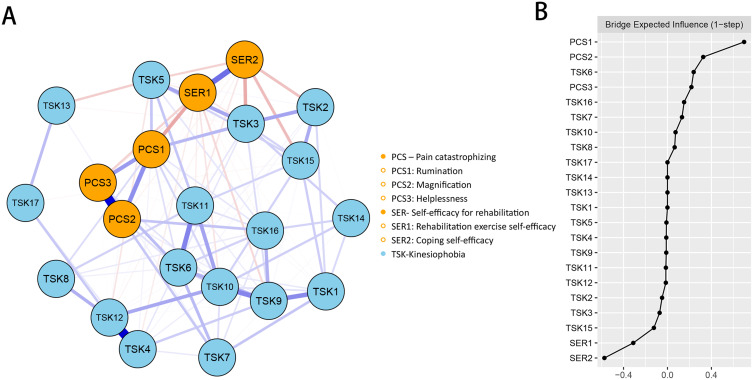
Methods: A total of 216 patients after total knee arthroplasty were recruited in this study. Pain Catastrophizing Scale, Self-efficacy of Rehabilitation Outcome Scale and Tampa Scale for Kinesiophobia were used to assess pain catastrophizing, self-efficacy and kinesiophobia. R software was used to visualize the networks and analyze the centrality of the networks. The index "strength" and "bridge expected influence" were employed to identify the central components and the bridge components of the networks.
Results: In the item network of kinesiophobia, three items ("Simply being careful that I do not make any unnecessary movements is the safest thing I can do to prevent my pain from worsening", "My accident has put my body at risk for the rest of my life", and "My body is telling me I have something dangerously wrong") had the highest strength centrality. In the pain catastrophizing/self-efficacy-kinesiophobia network, rumination had the highest positive bridge expected influence, while coping self-efficacy had the highest negative value.
Conclusion: The three central components of kinesiophobia identified in this study, as well as two bridge variables (rumination and coping self-efficacy), could be promising and effective targets for prevention and intervention of kinesiophobia.
Keywords: kinesiophobia; network analysis; pain catastrophizing; self-efficacy; total knee arthroplasty.
© 2024 Zhou et al.
Conflict of interest statement
The authors have no relevant competing interests to disclose in this work.
Figures
Similar articles
-
Pain Catastrophizing, Kinesiophobia and Exercise Adherence in Patients After Total Knee Arthroplasty: The Mediating Role of Exercise Self-Efficacy.J Pain Res. 2023 Nov 21;16:3993-4004. doi: 10.2147/JPR.S432106. eCollection 2023. J Pain Res. 2023. PMID: 38026453 Free PMC article.
-
Network analysis of perception of exercise benefits/barriers and kinesiophobia among patients with cardiovascular diseases.Heart Lung. 2024 Mar-Apr;64:182-188. doi: 10.1016/j.hrtlng.2023.12.006. Epub 2024 Jan 28. Heart Lung. 2024. PMID: 38281371
-
Pain and daily interference among reproductive-age women with myofascial pelvic pain: Serial mediation roles of kinesiophobia, self-efficacy and pain catastrophizing.PLoS One. 2024 May 13;19(5):e0301095. doi: 10.1371/journal.pone.0301095. eCollection 2024. PLoS One. 2024. PMID: 38739604 Free PMC article.
-
The relationship between pain catastrophizing, kinesiophobia and subjective knee function during rehabilitation following anterior cruciate ligament reconstruction and meniscectomy: A pilot study.Medicina (Kaunas). 2016;52(4):229-237. doi: 10.1016/j.medici.2016.07.005. Epub 2016 Aug 11. Medicina (Kaunas). 2016. PMID: 27623044
-
The Impact of Psychological Factors and Their Treatment on the Results of Total Knee Arthroplasty.J Bone Joint Surg Am. 2021 Sep 15;103(18):1744-1756. doi: 10.2106/JBJS.20.01479. J Bone Joint Surg Am. 2021. PMID: 34252068 Review.
Cited by
-
Beyond the Surgery: The Impact of Coping Strategies on Persistent Pain After Rotator Cuff Repair.J Clin Med. 2024 Nov 1;13(21):6584. doi: 10.3390/jcm13216584. J Clin Med. 2024. PMID: 39518724 Free PMC article.
References
-
- World Health Organization. Osteoarthritis; Available from: https://www.who.int/news-room/fact-sheets/detail/osteoarthritis.Accessed June 7 2024.
-
- Bian YY, Cheng KY, Chang X, Weng XS. Reports and analysis of amount of Hip and knee arthroplasty in China from 2011 to 2019. Chin J Orthop. 2020;40(21):1453–1460. doi:10.3760/cma.j.cn121113-20200320-00177 - DOI
-
- Bakaa N. Exercise adherence post total knee arthroplasty. McMaster Univ. 2020.
LinkOut - more resources
Full Text Sources
