

Theranostics with somatostatin receptor antagonists in SCLC: Correlation of 68Ga-SSO120 PET with immunohistochemistry and survival
- PMID: 39310095
- PMCID: PMC11413793
- DOI: 10.7150/thno.98819
Theranostics with somatostatin receptor antagonists in SCLC: Correlation of 68Ga-SSO120 PET with immunohistochemistry and survival
Abstract
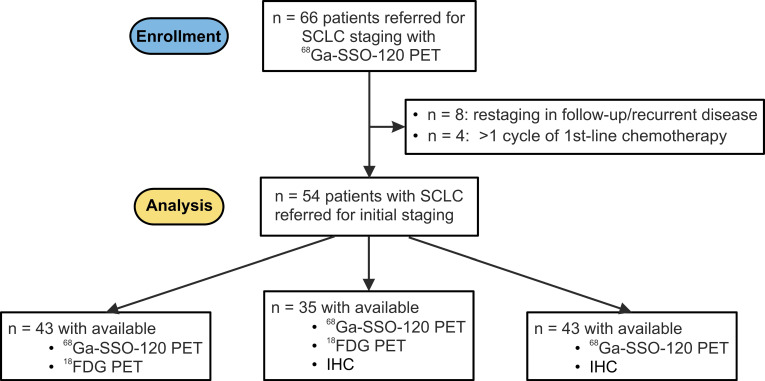
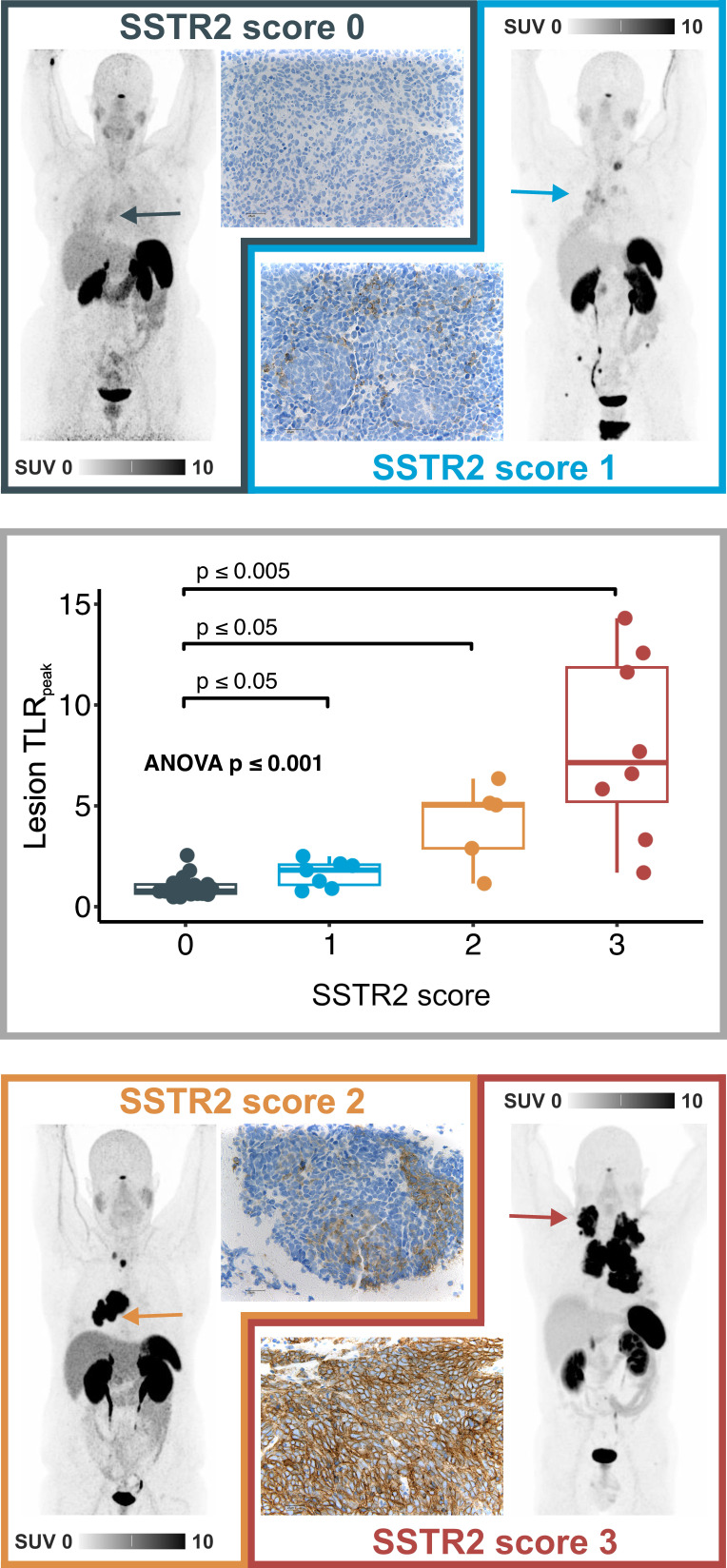
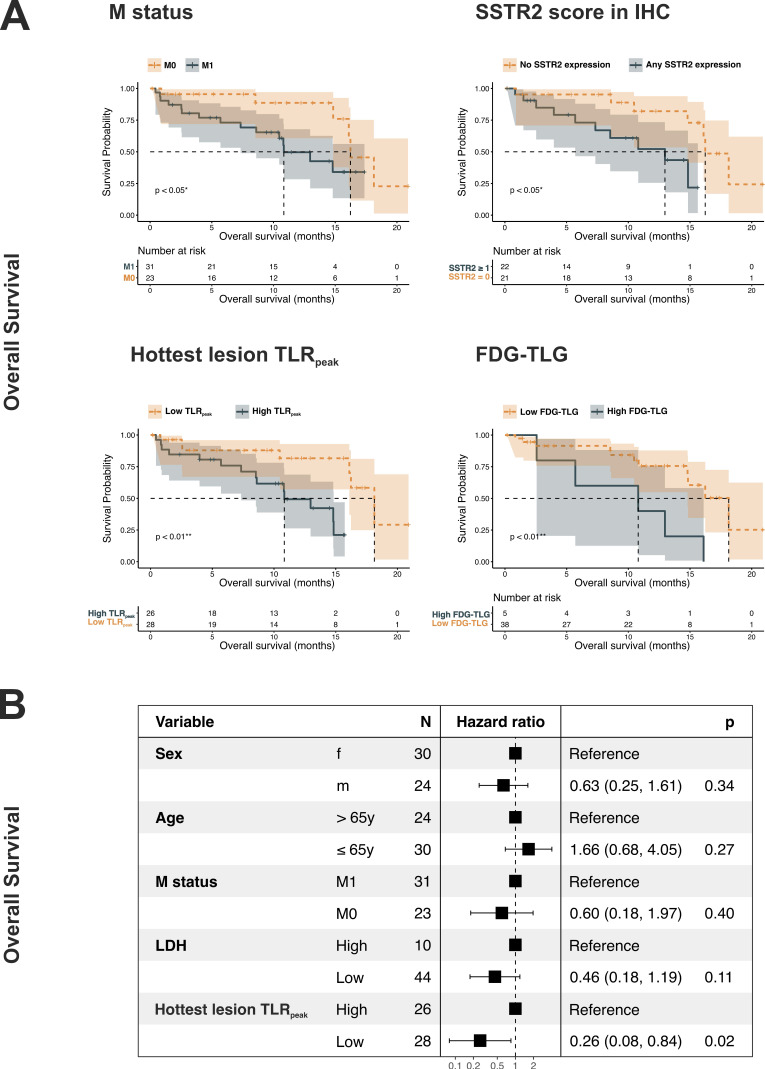
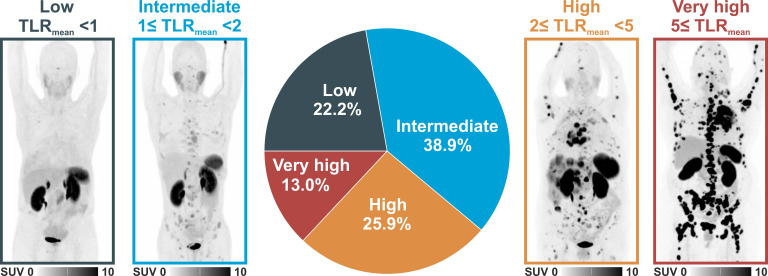
Rationale: Positron Emission Tomography (PET) using the somatostatin receptor 2 (SSTR2)-antagonist satoreotide trizoxetan (68Ga-SSO120) is a novel, promising imaging modality for small-cell lung cancer (SCLC), which holds potential for theranostic applications. This study aims to correlate uptake in PET imaging with SSTR2 expression in immunohistochemistry (IHC) and to assess the prognostic value of 68Ga-SSO120 PET at initial staging of patients with SCLC. Methods: We analyzed patients who underwent 68Ga-SSO120 PET/CT during initial diagnostic workup of SCLC as part of institutional standard-of-care. SSTR2 expression in IHC was evaluated on a 4-level scale and correlated with normalized standardized uptake values and tumor-to-liver ratios (SUVmax and TLRpeak) in 68Ga-SSO120 PET on a lesion level. Highest lesion SUVmax/TLRpeak per patient, SSTR2 score in IHC, M status according to TNM classification, and other parameters were analyzed for association with overall survival (OS) and time to treatment failure (TTF) by univariate, multivariate (cut-off values were identified on data for best separation), and stratified Cox regression. Results: We included 54 patients (24 men/30 women, median age 65 years, 21 M0/33 M1 according to TNM classification). In 43 patients with available surplus tumor tissue samples, hottest lesion SUVmax/TLRpeak showed a significant correlation with the level of SSTR2-expression by tumor cells in IHC (Spearman's rho 0.86/0.81, both p < 0.001; ANOVA p < 0.001). High SSTR2 expression in IHC, 68Ga-SSO120 SUVmax and TLRpeak of the hottest lesion per patient, whole-body TLRmean, MTV, TLG, M status, and serum LDH showed a significant association with inferior TTF/OS in univariate analysis. In separate multivariate Cox regression (including sex, age, M stage, and LDH) higher hottest-lesion TLRpeak showed a significant association with shorter OS (HR = 0.26, 95%CI: 0.08-0.84, p = 0.02) and SSTR2 expression in IHC with significantly shorter TTF (HR = 0.24, 95%CI: 0.08-0.71, p = 0.001) and OS (HR = 0.22, 95%CI: 0.06-0.84, p = 0.03). In total, 12 patients (22.2%) showed low (< 1), 21 (38.9%) intermediate (≥ 1 but < 2), 14 (25.9%) high (≥ 2 but < 5), and 7 (13.0%) very high (≥ 5) whole-body mean TLRmean. Conclusion: In patients with SCLC, SSTR2 expression assessed by 68Ga-SSO120 PET and by IHC were closely correlated and associated with shorter survival. More than 75% of patients showed higher whole-body 68Ga-SSO120 tumor uptake than liver uptake and almost 40% high or very high uptake, possibly paving the way towards theranostic applications.
Keywords: 68Ga-SSO120; IHC; PET; SCLC; SSTR.
© The author(s).
Conflict of interest statement
Competing Interests: Filiz Oezkan received personal fees from Sanofi Aventis, Janssen, DeciBio, ERBE and Genentech/Roche Ltd.; program funding to the institution was received from Olympus, Astrazeneca, ERBE and Janssen, all outside the submitted work. Lale Umutlu is a Speaker / Advisory Board Member for Bayer Healthcare and Siemens Healthcare and received research grants from Siemens Healthcare outside the submitted work. Rainer Hamacher was supported by the Clinician Scientist Program of the University Medicine Essen Clinician Scientist Academy (UMEA; Faculty of Medicine and Deutsche Forschungsgemeinschaft [DFG]); reports travel grants from Lilly, Novartis, and PharmaMar; and reports personal fees from Lilly and PharmaMar outside the submitted work. Jens Siveke is supported by German Cancer Aid (grant 70112505, PIPAC; grant 70113834, PREDICT-PACA), the Wilhelm-Sander Foundation (grant 2019.008.1), the DFG through grant SI1549/3-1 (Clinical Research Unit KFO337) and SI1549/4-1, and the Federal Ministry of Education and Research (BMBF; SATURN3 consortium); receives honoraria as a consultant or for continuing medical education presentations from AstraZeneca, Bayer, Immunocore, Roche, and Servier; receives research funding (to the institution) from Bristol Myers Squibb, Celgene, and Roche; and holds ownership and serves on the board of directors of Pharma15—all outside the submitted work. Wolfgang Fendler reports fees from SOFIE Biosciences (research funding), Janssen (consultant, speaker), Calyx (consultant, image review), Bayer (consultant, speaker, research funding), Novartis (speaker, consultant), Telix (speaker), GE Healthcare (speaker), Eczacıbaşı Monrol (speaker), Abx (speaker), Amgen (speaker), and Urotrials, all outside the submitted work. Marcel Wiesweg reports honoraria and advisory role from Amgen, AstraZeneca, Daiichi Sankyo, GlaxoSmithKline, Janssen, Novartis, Pfizer, Roche, Takeda, and research funding from Bristol-Myers Squibb, Takeda outside the submitted work. Ken Herrmann reports personal fees from Bayer, personal fees and other from Sofie Biosciences, personal fees from SIRTEX, non-financial support from ABX, personal fees from Adacap, personal fees from Curium, personal fees from Endocyte, grants and personal fees from BTG, personal fees from IPSEN, personal fees from Siemens Healthineers, personal fees from GE Healthcare, personal fees from Amgen, personal fees from Novartis, personal fees from ymabs, personal fees from Aktis Oncology, personal fees from Theragnostics, personal fees from Pharma15, outside the submitted work. Martin Schuler reports personal fees as a consultant from Amgen, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, GlaxoSmithKline, Janssen, Merck Serono, Novartis, Roche, Sanofi, and Takeda; honoraria for continuing medical education presentations from Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Janssen, MSD, and Novartis; and research funding (to the institution) from AstraZeneca and Bristol Myers Squibb, all outside the submitted work. Hubertus Hautzel reports personal fees from Roche and Urenco, and other fees from Pari, Roche and Urenco, outside the submitted work. David Kersting reports speaker honoraria from Pfizer and Novartis outside the submitted work. A research grant from Pfizer outside the submitted work and funding by the German Research Foundation (DFG, KE2933/1-1), outside the submitted work.
Figures
References
-
- Arnold C. Theranostics could be big business in precision oncology. Nat Med. 2022;28:606–8. - PubMed
-
- Basu S, Kwee TC, Gatenby R, Saboury B, Torigian DA, Alavi A. Evolving role of molecular imaging with PET in detecting and characterizing heterogeneity of cancer tissue at the primary and metastatic sites, a plausible explanation for failed attempts to cure malignant disorders. Eur J Nucl Med Mol Imaging. 2011;38:987–91. - PubMed
-
- Fischer BM, Mortensen J, Langer SW, Loft A, Berthelsen AK, Petersen BI. et al. A prospective study of PET/CT in initial staging of small-cell lung cancer: comparison with CT, bone scintigraphy and bone marrow analysis. Ann Oncol. 2007;18:338–45. - PubMed
-
- Fischer B, Lassen U, Mortensen J, Larsen S, Loft A, Bertelsen A. et al. Preoperative staging of lung cancer with combined PET-CT. N Engl J Med. 2009;361:32–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
