

Early versus delayed necrosectomy in pancreatic necrosis: A population-based cohort study on readmission, healthcare utilization, and in-hospital mortality
- PMID: 39310231
- PMCID: PMC11230070
- DOI: 10.5662/wjm.v14.i3.91810
Early versus delayed necrosectomy in pancreatic necrosis: A population-based cohort study on readmission, healthcare utilization, and in-hospital mortality
Abstract
Background: Acute necrotizing pancreatitis is a severe and life-threatening condition. It poses a considerable challenge for clinicians due to its complex nature and the high risk of complications. Several minimally invasive and open necrosectomy procedures have been developed. Despite advancements in treatment modalities, the optimal timing to perform necrosectomy lacks consensus.
Aim: To evaluate the impact of necrosectomy timing on patients with pancreatic necrosis in the United States.
Methods: A national retrospective cohort study was conducted using the 2016-2019 Nationwide Readmissions Database. Patients with non-elective admissions for pancreatic necrosis were identified. The participants were divided into two groups based on the necrosectomy timing: The early group received intervention within 48 hours, whereas the delayed group underwent the procedure after 48 hours. The various intervention techniques included endoscopic, percutaneous, or surgical necrosectomy. The major outcomes of interest were 30-day readmission rates, healthcare utilization, and inpatient mortality.
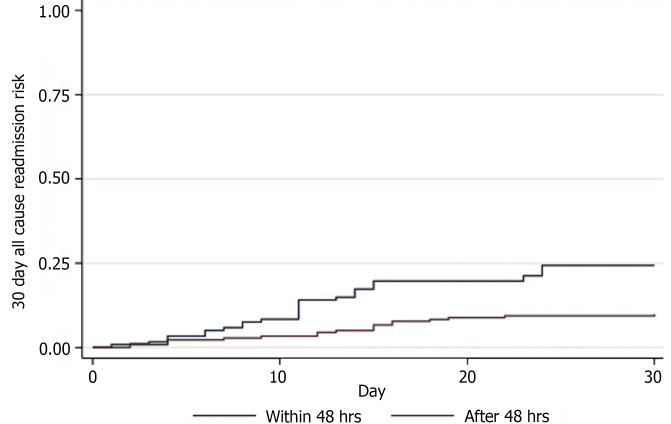
Results: A total of 1309 patients with pancreatic necrosis were included. After propensity score matching, 349 cases treated with early necrosectomy were matched to 375 controls who received delayed intervention. The early cohort had a 30-day readmission rate of 8.6% compared to 4.8% in the delayed cohort (P = 0.040). Early necrosectomy had lower rates of mechanical ventilation (2.9% vs 10.9%, P < 0.001), septic shock (8% vs 19.5%, P < 0.001), and in-hospital mortality (1.1% vs 4.3%, P = 0.01). Patients in the early intervention group incurred lower healthcare costs, with median total charges of $52202 compared to $147418 in the delayed group. Participants in the early cohort also had a relatively shorter median length of stay (6 vs 16 days, P < 0.001). The timing of necrosectomy did not significantly influence the risk of 30-day readmission, with a hazard ratio of 0.56 (95% confidence interval: 0.31-1.02, P = 0.06).
Conclusion: Our findings show that early necrosectomy is associated with better clinical outcomes and lower healthcare costs. Delayed intervention does not significantly alter the risk of 30-day readmission.
Keywords: Acute necrotizing pancreatitis; Delayed necrosectomy; Early necrosectomy; Mortality; Pancreatic necrosis; Readmission, Healthcare costs.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article. The preliminary form of these data was presented as an abstract at the Digestive Disease Week (DDW), May 19-21, 2024 in Washington, DC, United States.
Figures
Similar articles
-
Role of Necrosectomy in Necrotizing Pancreatitis: A Narrative Review.Cureus. 2024 Sep 29;16(9):e70470. doi: 10.7759/cureus.70470. eCollection 2024 Sep. Cureus. 2024. PMID: 39479145 Free PMC article. Review.
-
Association between acute peripancreatic fluid collections and early readmission in acute pancreatitis: A propensity-matched analysis.World J Exp Med. 2024 Jun 20;14(2):92052. doi: 10.5493/wjem.v14.i2.92052. eCollection 2024 Jun 20. World J Exp Med. 2024. PMID: 38948418 Free PMC article.
-
American Gastroenterological Association Clinical Practice Update: Management of Pancreatic Necrosis.Gastroenterology. 2020 Jan;158(1):67-75.e1. doi: 10.1053/j.gastro.2019.07.064. Epub 2019 Aug 31. Gastroenterology. 2020. PMID: 31479658 Review.
-
Safety of endoscopic pancreatic necrosectomy compared with percutaneous and surgical necrosectomy: a nationwide inpatient study.Endosc Int Open. 2023 Apr 4;11(4):E330-E339. doi: 10.1055/a-1994-6214. eCollection 2023 Apr. Endosc Int Open. 2023. PMID: 37025154 Free PMC article.
-
Minimally invasive and endoscopic versus open necrosectomy for necrotising pancreatitis: a pooled analysis of individual data for 1980 patients.Gut. 2018 Apr;67(4):697-706. doi: 10.1136/gutjnl-2016-313341. Epub 2017 Aug 3. Gut. 2018. PMID: 28774886
Cited by
-
Endoscopic management of infected necrotizing pancreatitis: Advancing through standardization.World J Gastroenterol. 2025 May 28;31(20):107451. doi: 10.3748/wjg.v31.i20.107451. World J Gastroenterol. 2025. PMID: 40495946 Free PMC article. Review.
-
Acute Necrotizing Pancreatitis-Advances and Challenges in Management for Optimal Clinical Outcomes.Medicina (Kaunas). 2025 Jun 30;61(7):1186. doi: 10.3390/medicina61071186. Medicina (Kaunas). 2025. PMID: 40731816 Free PMC article. Review.
-
Role of Necrosectomy in Necrotizing Pancreatitis: A Narrative Review.Cureus. 2024 Sep 29;16(9):e70470. doi: 10.7759/cureus.70470. eCollection 2024 Sep. Cureus. 2024. PMID: 39479145 Free PMC article. Review.
-
Analysis of risk factors for elective surgery complications in a cancer specialty hospital based on propensity score matching.BMC Health Serv Res. 2025 Jul 1;25(1):834. doi: 10.1186/s12913-025-13065-1. BMC Health Serv Res. 2025. PMID: 40598283 Free PMC article.
References
-
- Peery AF, Crockett SD, Murphy CC, Jensen ET, Kim HP, Egberg MD, Lund JL, Moon AM, Pate V, Barnes EL, Schlusser CL, Baron TH, Shaheen NJ, Sandler RS. Burden and Cost of Gastrointestinal, Liver, and Pancreatic Diseases in the United States: Update 2021. Gastroenterology. 2022;162:621–644. - PMC - PubMed
-
- Boxhoorn L, Voermans RP, Bouwense SA, Bruno MJ, Verdonk RC, Boermeester MA, van Santvoort HC, Besselink MG. Acute pancreatitis. Lancet. 2020;396:726–734. - PubMed
-
- van Santvoort HC, Bakker OJ, Bollen TL, Besselink MG, Ahmed Ali U, Schrijver AM, Boermeester MA, van Goor H, Dejong CH, van Eijck CH, van Ramshorst B, Schaapherder AF, van der Harst E, Hofker S, Nieuwenhuijs VB, Brink MA, Kruyt PM, Manusama ER, van der Schelling GP, Karsten T, Hesselink EJ, van Laarhoven CJ, Rosman C, Bosscha K, de Wit RJ, Houdijk AP, Cuesta MA, Wahab PJ, Gooszen HG Dutch Pancreatitis Study Group. A conservative and minimally invasive approach to necrotizing pancreatitis improves outcome. Gastroenterology. 2011;141:1254–1263. - PubMed
-
- Trikudanathan G, Wolbrink DRJ, van Santvoort HC, Mallery S, Freeman M, Besselink MG. Current Concepts in Severe Acute and Necrotizing Pancreatitis: An Evidence-Based Approach. Gastroenterology. 2019;156:1994–2007.e3. - PubMed
LinkOut - more resources
Full Text Sources
