

Anticoagulant use before COVID-19 diagnosis prevent COVID-19 associated acute venous thromboembolism or not: A systematic review and meta-analysis
- PMID: 39310244
- PMCID: PMC11230074
- DOI: 10.5662/wjm.v14.i3.92983
Anticoagulant use before COVID-19 diagnosis prevent COVID-19 associated acute venous thromboembolism or not: A systematic review and meta-analysis
Abstract
Background: Coagulopathy and thromboembolic events are associated with poor outcomes in coronavirus disease 2019 (COVID-19) patients. There is conflicting evidence on the effects of chronic anticoagulation on mortality and severity of COVID-19 disease.
Aim: To summarize the body of evidence on the effects of pre-hospital anticoagulation on outcomes in COVID-19 patients.
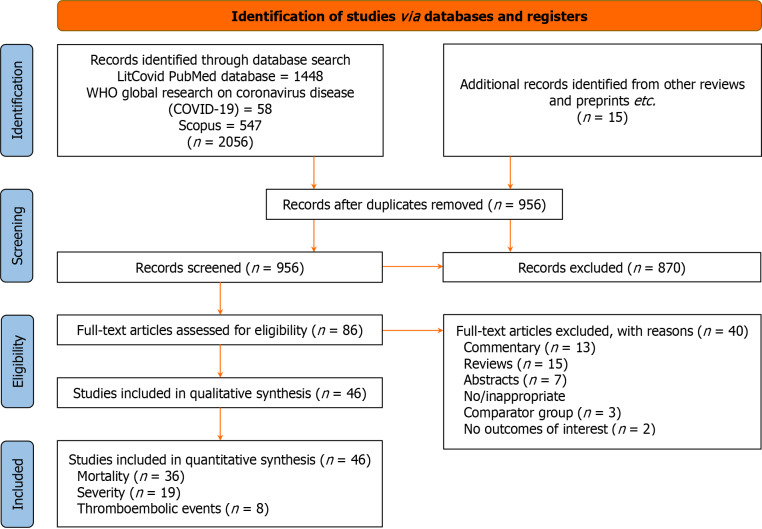
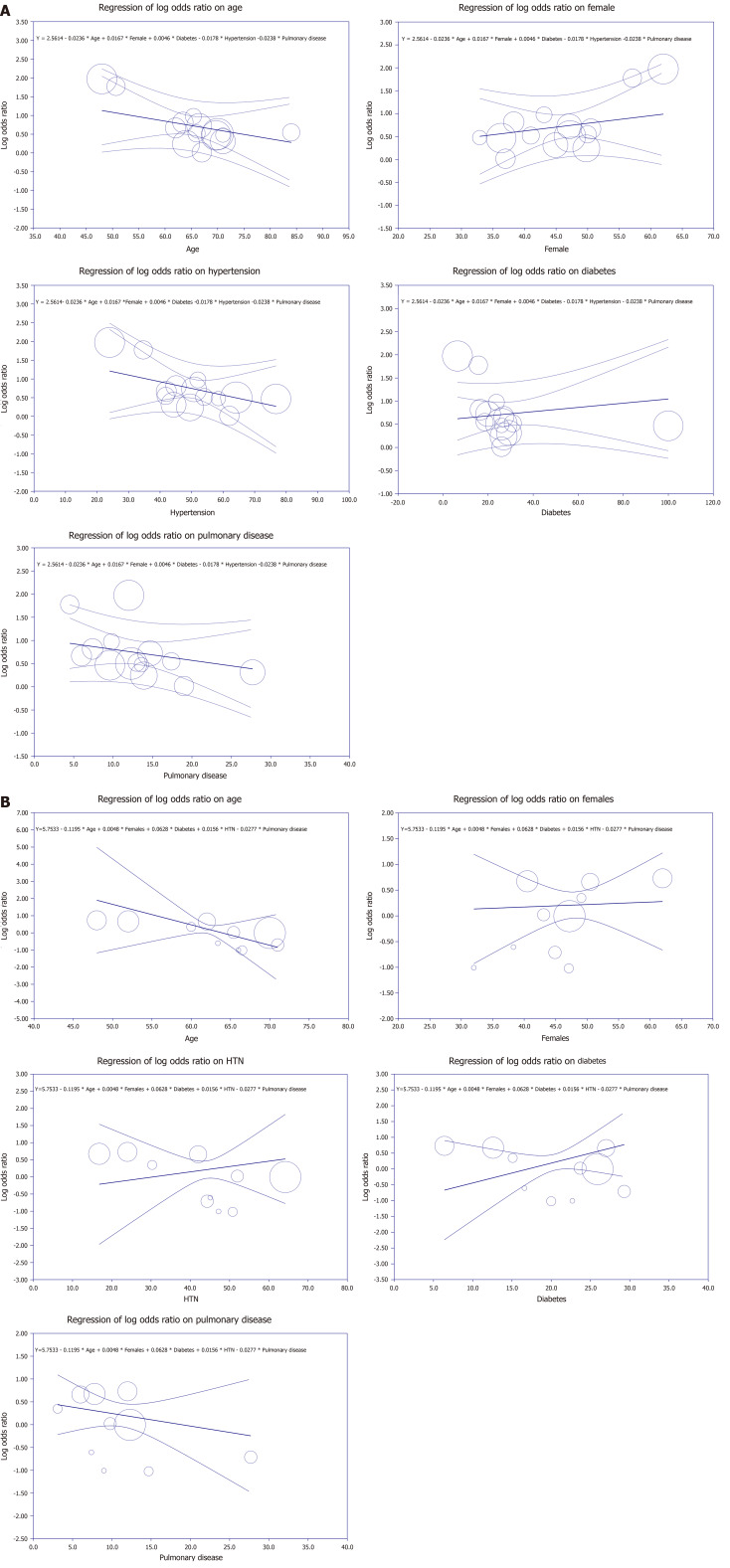
Methods: A Literature search was performed on LitCovid PubMed, WHO, and Scopus databases from inception (December 2019) till June 2023 for original studies reporting an association between prior use of anticoagulants and patient outcomes in adults with COVID-19. The primary outcome was the risk of thromboembolic events in COVID-19 patients taking anticoagulants. Secondary outcomes included COVID-19 disease severity, in terms of intensive care unit admission or invasive mechanical ventilation/intubation requirement in patients hospitalized with COVID-19 infection, and mortality. The random effects models were used to calculate crude and adjusted odds ratios (aORs) with 95% confidence intervals (95%CIs).
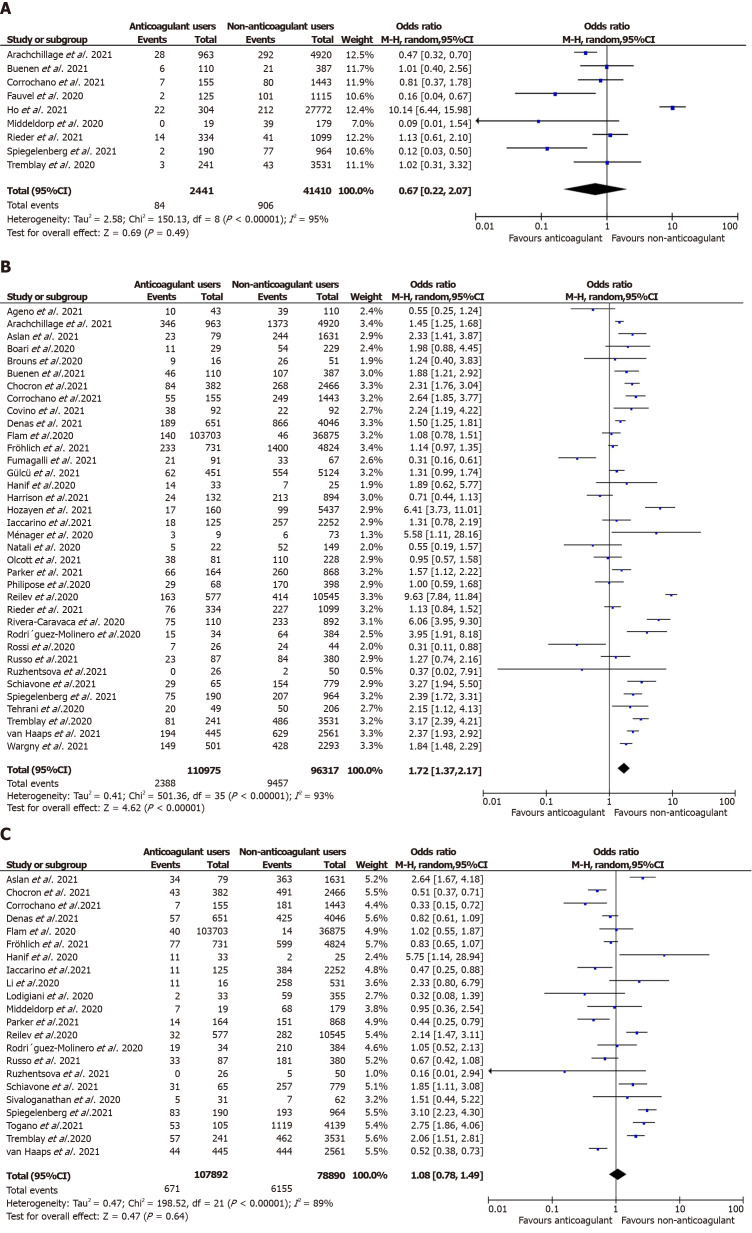
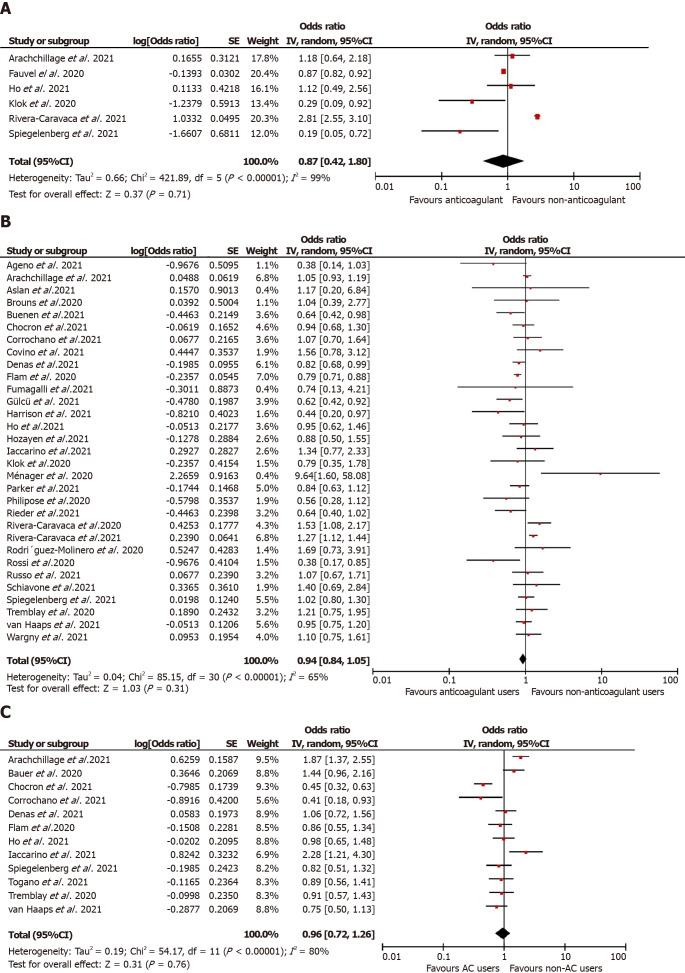
Results: Forty-six observational studies met our inclusion criteria. The unadjusted analysis found no association between prior anticoagulation and thromboembolic event risk [n = 43851, 9 studies, odds ratio (OR)= 0.67 (0.22, 2.07); P = 0.49; I 2 = 95%]. The association between prior anticoagulation and disease severity was non-significant [n = 186782; 22 studies, OR = 1.08 (0.78, 1.49); P = 0.64; I 2 = 89%]. However, pre-hospital anticoagulation significantly increased all-cause mortality risk [n = 207292; 35 studies, OR = 1.72 (1.37, 2.17); P < 0.00001; I 2 = 93%]. Pooling adjusted estimates revealed a statistically non-significant association between pre-hospital anticoagulation and thromboembolic event risk [aOR = 0.87 (0.42, 1.80); P = 0.71], mortality [aOR = 0.94 (0.84, 1.05); P = 0.31], and disease severity [aOR = 0.96 (0.72, 1.26); P = 0.76].
Conclusion: Prehospital anticoagulation was not significantly associated with reduced risk of thromboembolic events, improved survival, and lower disease severity in COVID-19 patients.
Keywords: COVID-19; Chronic anticoagulation; Mortality; Prehospital anticoagulation; Prior anticoagulation; Severity; Thromboembolic events.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: Dr. Bansal has nothing to disclose.
Figures
Similar articles
-
Prophylactic anticoagulants for people hospitalised with COVID-19.Cochrane Database Syst Rev. 2020 Oct 2;10(10):CD013739. doi: 10.1002/14651858.CD013739. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2022 Mar 4;3:CD013739. doi: 10.1002/14651858.CD013739.pub2. PMID: 33502773 Free PMC article. Updated.
-
Point-of-Care International Normalized Ratio (INR) Monitoring Devices for Patients on Long-term Oral Anticoagulation Therapy: An Evidence-Based Analysis.Ont Health Technol Assess Ser. 2009;9(12):1-114. Epub 2009 Sep 1. Ont Health Technol Assess Ser. 2009. PMID: 23074516 Free PMC article.
-
Randomised controlled trial comparing efficacy and safety of high versus low Low-Molecular Weight Heparin dosages in hospitalized patients with severe COVID-19 pneumonia and coagulopathy not requiring invasive mechanical ventilation (COVID-19 HD): a structured summary of a study protocol.Trials. 2020 Jun 26;21(1):574. doi: 10.1186/s13063-020-04475-z. Trials. 2020. PMID: 32586394 Free PMC article.
-
The impact of pre-injury anticoagulation therapy in the older adult patient experiencing a traumatic brain injury: A systematic review.JBI Libr Syst Rev. 2012;10(58):4610-4621. doi: 10.11124/jbisrir-2012-429. JBI Libr Syst Rev. 2012. PMID: 27820526
-
Anticoagulation outcomes in hospitalized Covid-19 patients: A systematic review and meta-analysis of case-control and cohort studies.Rev Med Virol. 2021 May;31(3):e2180. doi: 10.1002/rmv.2180. Epub 2020 Oct 6. Rev Med Virol. 2021. PMID: 33022834 Free PMC article.
References
-
- Rathore SS, Rojas GA, Sondhi M, Pothuru S, Pydi R, Kancherla N, Singh R, Ahmed NK, Shah J, Tousif S, Baloch UT, Wen Q. Myocarditis associated with Covid-19 disease: A systematic review of published case reports and case series. Int J Clin Pract. 2021;75:e14470. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
