

Infarct of the Middle Cerebellar Peduncle Mimicking Bell's Palsy: A Case Report
- PMID: 39310426
- PMCID: PMC11416183
- DOI: 10.7759/cureus.67533
Infarct of the Middle Cerebellar Peduncle Mimicking Bell's Palsy: A Case Report
Abstract
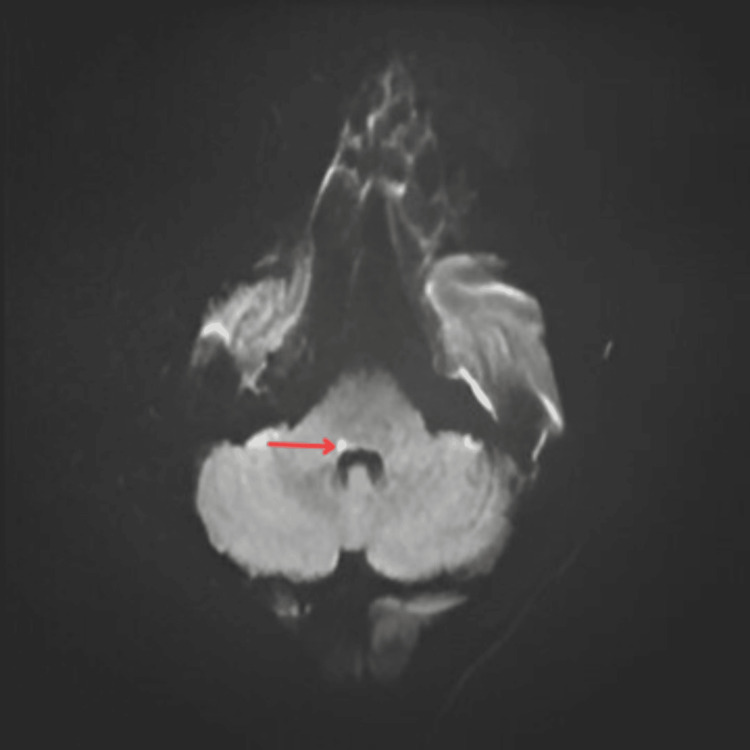
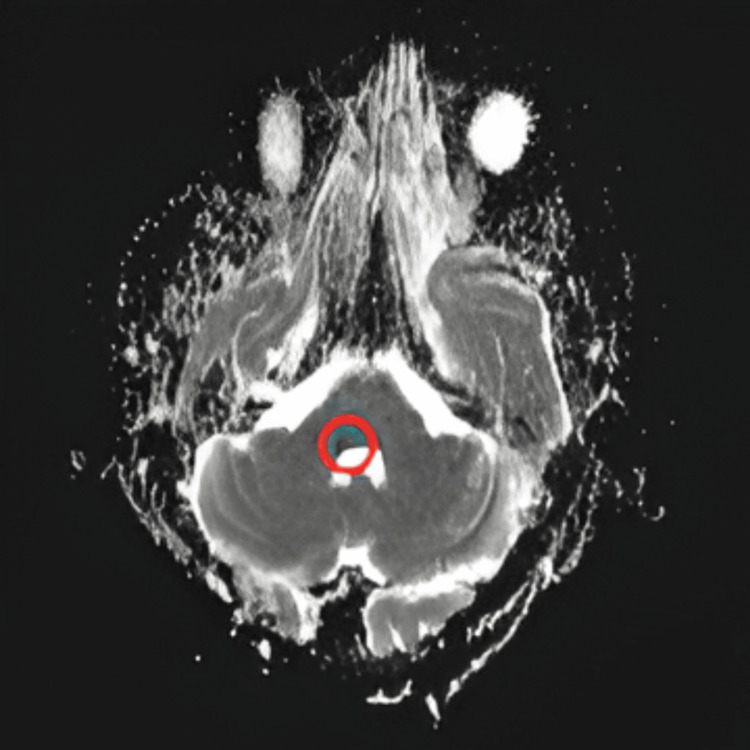
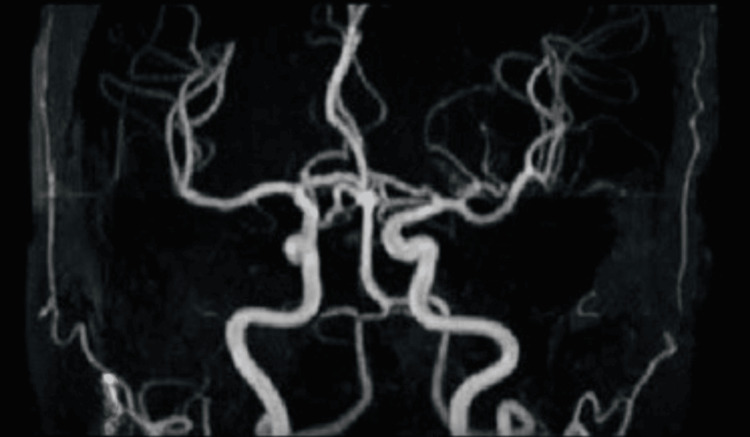
The anterior inferior cerebellar artery (AICA) supplies the middle cerebellar peduncle, lower pons, upper medulla, and anterior inferior cerebellum. Ischemia in the AICA can cause the lateral inferior pontine syndrome. AICA syndrome is characterized by facial sensory loss and weakness, Horner syndrome, prolonged vertigo, audio-vestibular loss, and cerebellar signs. Many studies on AICA territory infarcts have demonstrated the rarity of complete AICA syndrome. In all cases of AICA territory infarcts, involvement of the middle cerebellar peduncle was observed, with the seventh cranial nerve (facial nerve) being the most frequently involved cranial nerve, vertigo was the most common presenting symptom, and atherosclerosis was the most common etiology. This case report aims to investigate the occurrence of middle cerebellar peduncle infarcts that mimic Bell's palsy, highlighting the importance of accurate diagnosis and appropriate management in such cases. Recognizing the unique characteristics and clinical presentation of middle cerebellar peduncle (MCP) infarcts is essential for distinguishing them from more common conditions like Bell's palsy, thereby ensuring timely and effective treatment.
Keywords: anterior inferior cerebellar artery; anterior inferior cerebellar artery syndrome; bell's palsy; lower motor neuron palsy; middle cerebellar peduncle infarct.
Copyright © 2024, Pandian et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. SRM Medical College Hospital and Research Centre issued approval NA. The investigator has got an approved consent from the patient to use the face of the patient in the image (Figure 1), as masking the identity in this case representing Bell's phenomenon will hide the findings. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures

References
-
- Baseline cerebro-cerebellar functional connectivity in afferent and efferent pathways reveal dissociable improvements in visuomotor learning. Lin YC, Lien YR, Lin SH, et al. https://www.frontiersin.org/journals/neuroscience/articles/10.3389/fnins.... Frontiers in Neuroscience. 2022;16:904564. - PMC - PubMed
-
- Isolated bilateral middle cerebellar peduncle infarcts. John S, Hegazy M, Cheng Ching E, Katzan I. J Stroke Cerebrovasc Dis. 2013;22:0–6. - PubMed
-
- Wallerian degeneration of the bilateral middle cerebellar peduncles secondary to pontine infarction. Shen Y, Nie H. https://link.springer.com/article/10.1007/s10072-017-3237-6. Neurol Sci. 2018;39:961–963. - PubMed
-
- Clinical study of seven patients with infarction in territories of the anterior inferior cerebellar artery. Ogawa K, Suzuki Y, Takahashi K, Akimoto T, Kamei S, Soma M. J Stroke Cerebrovasc Dis. 2017;26:574–581. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous