

Persistent Mycobacterium tuberculosis bioaerosol release in a tuberculosis-endemic setting
- PMID: 39310776
- PMCID: PMC11414687
- DOI: 10.1016/j.isci.2024.110731
Persistent Mycobacterium tuberculosis bioaerosol release in a tuberculosis-endemic setting
Abstract
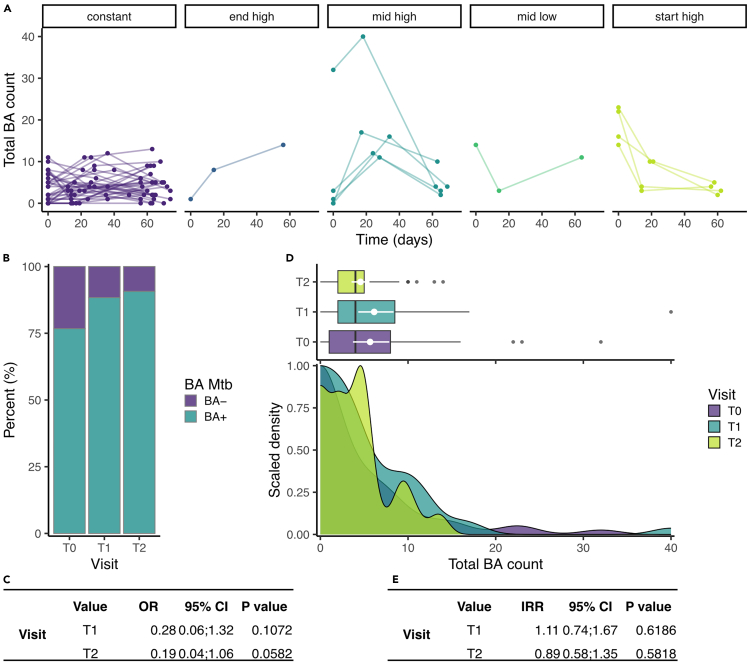
Pioneering studies linking symptomatic disease and cough-mediated Mycobacterium tuberculosis (Mtb) release established the infectious origin of tuberculosis (TB), simultaneously informing the notion that pathology is a prerequisite for Mtb transmission. Our recent work has challenged this assumption: by sampling TB clinic attendees, we detected equivalent release of Mtb-containing bioaerosols by confirmed TB patients and individuals not receiving a TB diagnosis and observed time-dependent reduction in Mtb bioaerosol positivity during 6-month follow-up of both cohorts, irrespective of anti-TB chemotherapy. Now, we report widespread Mtb release in our TB-endemic setting: of 89 randomly recruited community members, 79.8% (71/89) produced Mtb-containing bioaerosols independently of QuantiFERON status, a standard test for Mtb exposure. Moreover, during 2-month longitudinal sampling, only 2% (1/50) were serially Mtb bioaerosol negative. These results necessitate a reframing of the prevailing paradigm of Mtb transmission and TB etiology, perhaps explaining the historical inability to elucidate Mtb transmission networks in TB-endemic regions.
Keywords: Microbiology.
© 2024 The Authors.
Conflict of interest statement
The authors have no conflicting interests to declare.
Figures





Update of
-
Persistent Mycobacterium tuberculosis bioaerosol release in a tuberculosis-endemic setting.medRxiv [Preprint]. 2024 Apr 3:2024.04.02.24305196. doi: 10.1101/2024.04.02.24305196. medRxiv. 2024. Update in: iScience. 2024 Aug 20;27(9):110731. doi: 10.1016/j.isci.2024.110731. PMID: 38633787 Free PMC article. Updated. Preprint.
References
-
- Drain P.K., Bajema K.L., Dowdy D., Dheda K., Naidoo K., Schumacher S.G., Ma S., Meermeier E., Lewinsohn D.M., Sherman D.R. Incipient and Subclinical Tuberculosis: a Clinical Review of Early Stages and Progression of Infection. Clin. Microbiol. Rev. 2018;31 doi: 10.1128/CMR.00021-18. - DOI - PMC - PubMed
-
- Coussens A.K., Zaidi S.M.A., Allwood B.W., Dewan P.K., Gray G., Kohli M., Kredo T., Marais B.J., Marks G.B., Martinez L., et al. Classification of early tuberculosis states to guide research for improved care and prevention: an international Delphi consensus exercise. Lancet Respir. Med. 2024;12:484–498. doi: 10.1016/S2213-2600(24)00028-6. - DOI - PMC - PubMed
-
- Richards A.S., Sossen B., Emery J.C., Horton K.C., Heinsohn T., Frascella B., Balzarini F., Oradini-Alacreu A., Häcker B., Odone A., et al. Quantifying progression and regression across the spectrum of pulmonary tuberculosis: a data synthesis study. Lancet Global Health. 2023;11:e684–e692. doi: 10.1016/S2214-109X(23)00082-7. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
