

The global burden of maternal disorders attributable to iron deficiency related sub-disorders in 204 countries and territories: an analysis for the Global Burden of Disease study
- PMID: 39310906
- PMCID: PMC11413869
- DOI: 10.3389/fpubh.2024.1406549
The global burden of maternal disorders attributable to iron deficiency related sub-disorders in 204 countries and territories: an analysis for the Global Burden of Disease study
Abstract
Background: Pregnancy-related anemia presents a significant health concern for approximately 500 million women of reproductive age worldwide. To better prevent maternal disorders, it is essential to understand the impact of iron deficiency across different maternal disorders, regions, age groups, and subcategories.
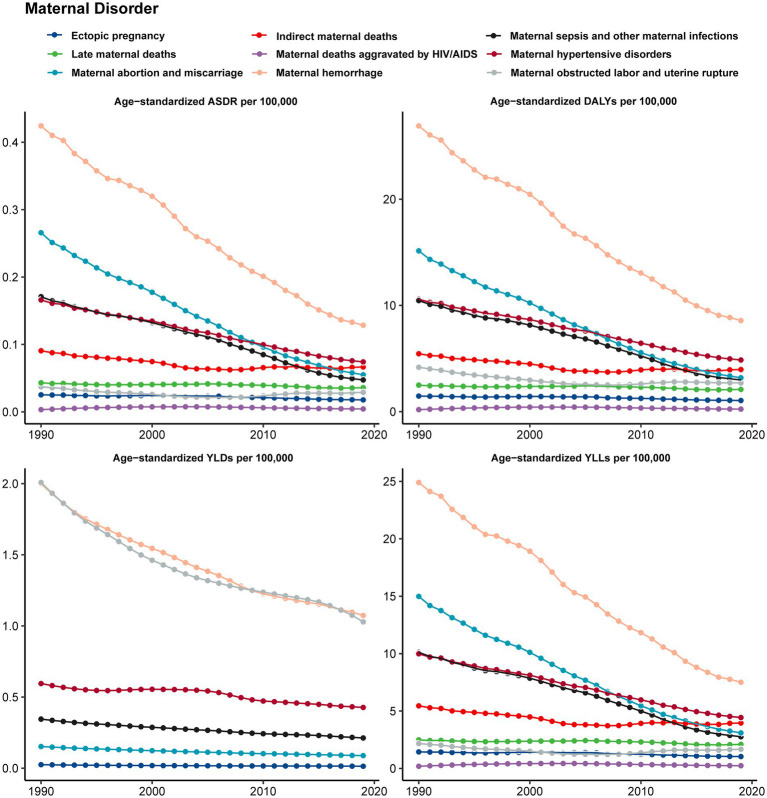
Methods: Based on the comprehensive maternal disorders data sourced from the 2019 Global Burden of Disease study, an investigation was carried out focusing on Disability-Adjusted Life Years (DALYs) associated with iron deficiency spanning the period from 1990 to 2019. In addition, Estimated Annual Percentage Changes (EAPCs) were computed for the duration of the study.
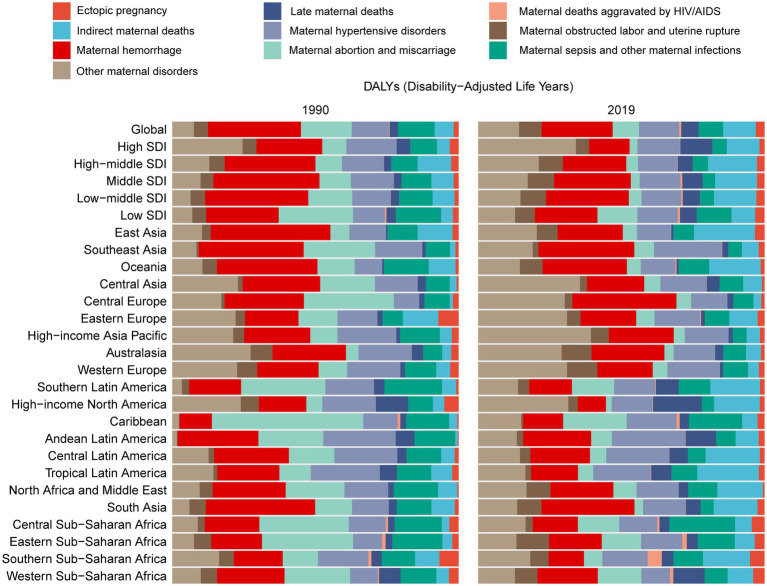
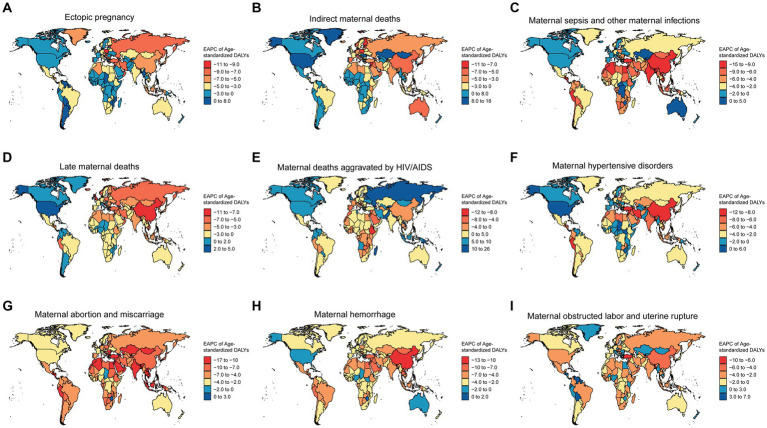
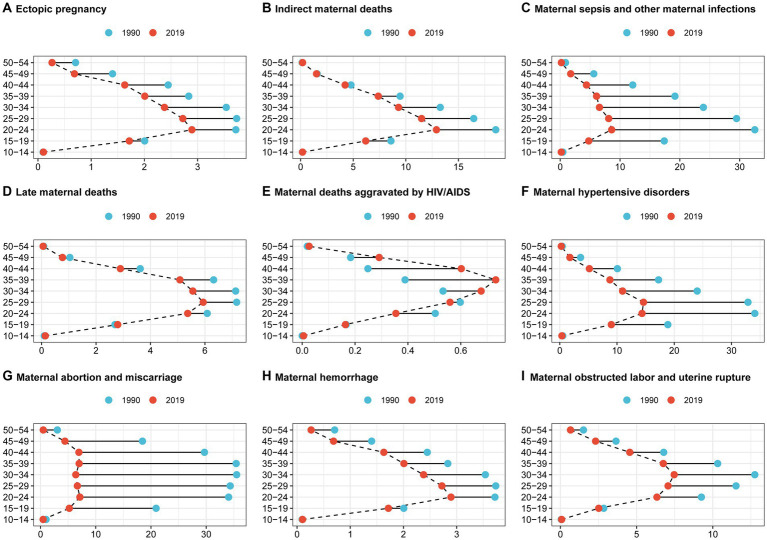
Results: Our study indicates decreasing mortality rates and years of life lost due to maternal conditions related to iron deficiency, such as maternal hemorrhage, miscarriage, abortion, hypertensive disorders, and infections. However, mortality rates and years of life lost due to indirect and late maternal deaths, as well as deaths aggravated by HIV/AIDS, have increased in high socio-demographic index (SDI) regions, especially in North America. Moreover, the proportion of maternal deaths aggravated by HIV/AIDS due to iron deficiency is rising globally, especially in Southern Sub-Saharan Africa, Oceania, and Georgia. In addition, in the Maldives, the age-standardized DALYs for maternal disorders attributable to iron deficiency exhibited a notable decreasing trend, encompassing a range of conditions. Furthermore, there was a significant decrease in Disability-Adjusted Life Years rate for miscarriages and preterm births among women aged 15-49, with hypertensive disorders posing the highest burden among women aged 15-39.
Conclusion: The burden of maternal disorders caused by iron deficiency is decreasing in most regions and subtypes, except for deaths aggravated by HIV/AIDS. By thoroughly understanding the details of how iron deficiency impacts the health of pregnant women, health policymakers, healthcare professionals, and researchers can more effectively pinpoint and address the root causes of inequalities in maternal health.
Keywords: Disability-Adjusted Life Years; Estimated Annual Percentage Changes; GBD 2019; iron deficiency; maternal disorders.
Copyright © 2024 Wu, Ye, Ba, Caikai, Ba, Li and Zhu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Organization Health W . Trends in maternal mortality 2000 to 2017: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. (2019).
-
- Alliance for Maternal and Newborn Health Improvement (AMANHI) Maternal Morbidity Study Group . Direct maternal morbidity and the risk of pregnancy-related deaths, stillbirths, and neonatal deaths in South Asia and sub-Saharan Africa: a population.
-
- Health Organization W . Trends in maternal mortality 2000 to 2017: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations population division: executive …. apps. who. int. (2019). Available at: https://apps.who.int/iris/bitstream/handle/10665/327596/WHO-RHR-19.23-ru... (Accessed March 10, 2024).
MeSH terms
LinkOut - more resources
Full Text Sources