

Intraductal Papillary Neoplasms of the Bile Duct: Clinical Case Insights and Literature Review
- PMID: 39311283
- PMCID: PMC11417733
- DOI: 10.3390/clinpract14050133
Intraductal Papillary Neoplasms of the Bile Duct: Clinical Case Insights and Literature Review
Abstract
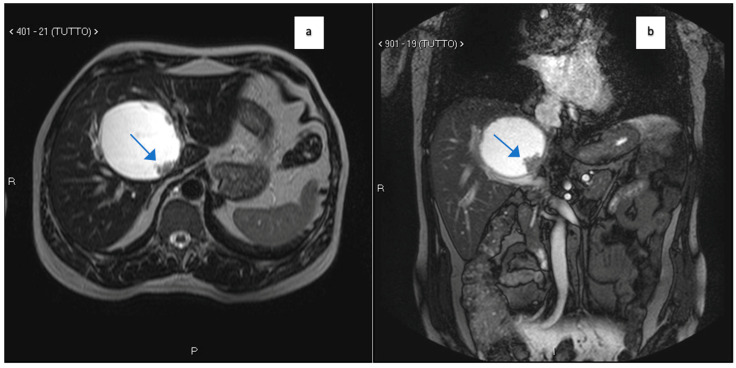
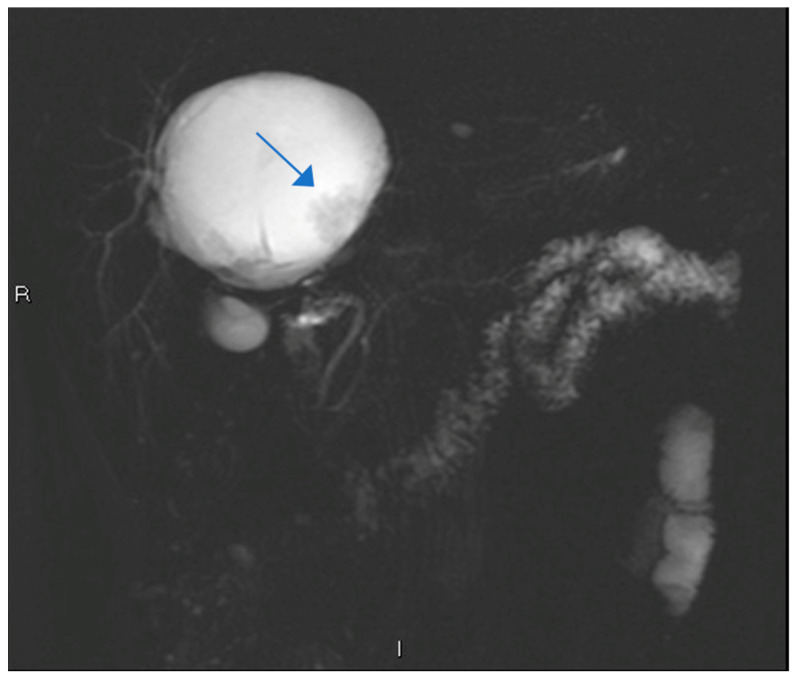
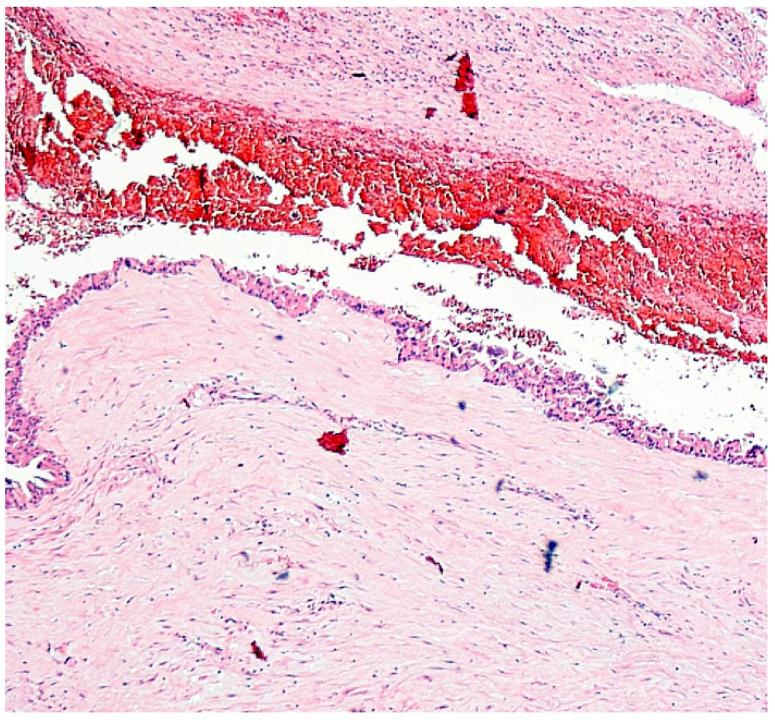
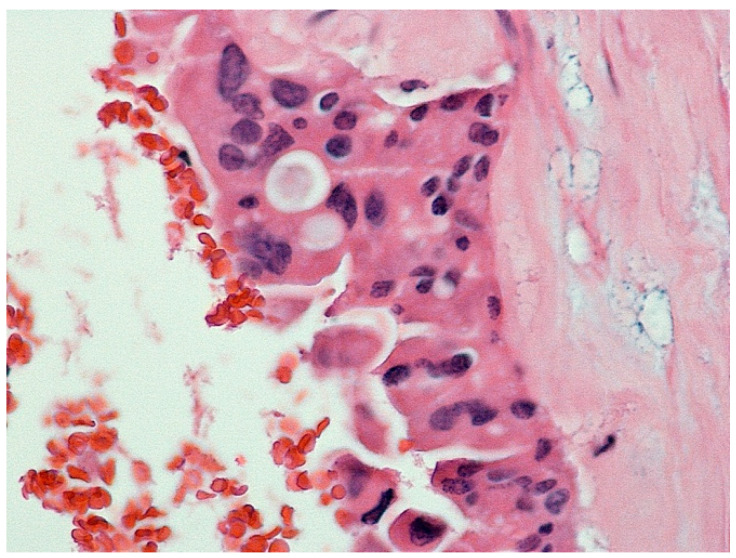
Background: Intraductal papillary neoplasms of the bile duct (IPNB) are rare precancerous lesions with implications for the development of cholangiocarcinoma (CCA). Recognizing IPNB and managing its recurrence pose challenges in clinical practice. We present two cases. Case 1: a 60-year-old man presented with an 8 × 8 × 9 cm hepatic cyst initially suspected to be a hydatid cyst. Histology post-resection revealed an IPNB with foci of adenocarcinoma. Despite negative oncologic margins, recurrence occurred eight years later as an rT2N0 lesion. Surgical resection was performed without adjuvant chemotherapy, resulting in the patient's survival at 48 months post-surgery. Case 2: a 28-year-old female with cognitive impairment was admitted with pulmonary embolism and a liver lesion diagnosed as a simple cyst. Subsequent evaluation revealed adenocarcinoma with local metastases, extensive vascular involvement, and thrombosis. Despite aggressive management, including thrombectomy and chemotherapy, the patient's condition deteriorated, leading to hepatic failure and eventual demise.
Conclusion: IPNB represents a rare premalignant subtype with a propensity for progression to CCA. R0 surgical resection typically offers favorable oncological outcomes with a minimal recurrence risk. Surgical intervention for localized resectable recurrence is both safe and feasible. International registries tracking IPNB recurrence are essential for advancing understanding and optimizing diagnosis, management, and treatment strategies.
Keywords: cholangiocarcinoma; intraductal papillary neoplasm of the bile duct; liver resection.
Conflict of interest statement
All authors have no conflicts of interest to declare.
Figures
References
-
- Zen Y., Sasaki M., Fujii T., Chen T.C., Chen M.F., Yeh T.S., Jan Y.Y., Huang S.F., Nimura Y., Nakanuma Y. Different expression patterns of mucin core proteins and cytokeratins during intrahepatic cholangiocarcinogenesis from biliary intraepithelial neoplasia and intraductal papillary neoplasm of the bile duct—An immunohistochemical study of 110 cases of hepatolithiasis. J. Hepatol. 2006;44:350–358. doi: 10.1016/j.jhep.2005.09.025. - DOI - PubMed
-
- Nanashima A., Imamura N., Hiyoshi M., Hamada T., Yano K., Wada T., Kawakami H., Ban T., Kubota Y., Sato Y., et al. Planned limited resection of the extrahepatic bile duct in a case of intraductal papillary neoplasm of the bile duct based on preoperative examinations. Clin. J. Gastroenterol. 2020;13:233–239. doi: 10.1007/s12328-019-01049-8. - DOI - PubMed
-
- Rocha F.G., Lee H., Katabi N., DeMatteo R.P., Fong Y., D’Angelica M.I., Allen P.J., Klimstra D.S., Jarnagin W.R. Intraductal papillary neoplasm of the bile duct: A biliary equivalent to intraductal papillary mucinous neoplasm of the pancreas? Hepatology. 2012;56:1352–1360. doi: 10.1002/hep.25786. - DOI - PubMed
-
- Harada F., Matsuyama R., Mori R., Kumamoto T., Morioka D., Taguri M., Yamanaka S., Endo I. Outcomes of surgery for 2010 WHO classification-based intraductal papillary neoplasm of the bile duct: Case-control study of a single Japanese institution’s experience with special attention to mucin expression patterns. Eur. J. Surg. Oncol. 2019;45:761–768. doi: 10.1016/j.ejso.2018.10.532. - DOI - PubMed
-
- Nakanuma Y., Uesaka K., Kakuda Y., Sugino T., Kubota K., Furukawa T., Fukumura Y., Isayama H., Terada T. Intraductal Papillary Neoplasm of Bile Duct: Updated Clinicopathological Characteristics and Molecular and Genetic Alterations. J. Clin. Med. 2020;9:3991. doi: 10.3390/jcm9123991. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
