

Pharmacologic evaluation of delayed long-acting cabotegravir administration among cisgender women in HPTN 084
- PMID: 39311597
- PMCID: PMC11539227
- DOI: 10.1128/aac.00994-24
Pharmacologic evaluation of delayed long-acting cabotegravir administration among cisgender women in HPTN 084
Abstract
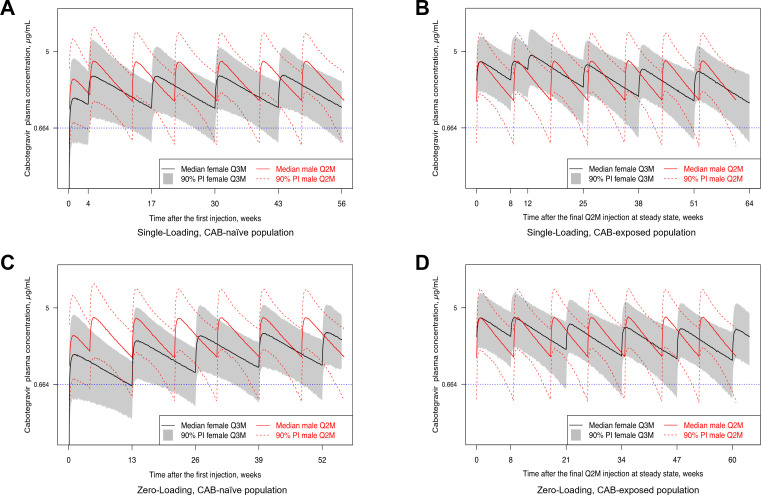
HPTN 084 demonstrated the superiority of long-acting injectable cabotegravir (CAB-LA) compared with daily oral tenofovir disoproxil fumarate-emtricitabine (F/TDF) for HIV prevention in women. CAB-LA (600 mg) or placebo injections were administered 4 weeks after an initial dose (loading dose) and every 2 months (Q2M) thereafter; this is the approved regimen. Participants experienced both loading dose and Q2M delays during the trial. CAB concentrations were evaluated before a delay, at the visit associated with the delay, and the visit after a delayed injection was administered. During the blinded phase of the trial, 194 participants randomized to CAB-LA experienced at least one injection delay. Plasma CAB concentrations were maintained above the 4× protein adjusted 90% inhibitory concentration (4× PA-IC90; protocol-specific threshold) for all loading dose and 98% of Q2M delays when injections were administered up to 6 weeks late. The feasibility of shifting to an every 3-month (Q3M) regimen in females was interrogated via simulation studies using a population pharmacokinetic model. Q3M injections in both CAB-naïve (with a loading dose) and previously CAB-exposed females were predicted to yield higher steady-state exposures than in males on the approved Q2M regimen. Although there is observed forgiveness following an isolated delayed CAB-LA injection and simulations suggest acceptable CAB-LA exposures in women with a 600 mg CAB-LA Q3M regimen, empirical efficacy of this regimen has not been established, and transitioning to this dosing schema is not recommended. Future pharmacokinetic bridging studies are aimed at evaluating higher dose CAB-LA formulations administered less frequently.
Clinical trials: This study is registered with ClinicalTrials.gov as NCT03164564.
Keywords: HIV; cabotegravir; modeling; pharmacokinetics; prevention.
Conflict of interest statement
K.H. and S.L.F. are employees and stockholders of GSK. A.R.R. is an employee of ViiV Healthcare and holds stock in GSK. J.F.R. is a paid employee of Gilead Sciences.
Figures



References
-
- Overton ET, Richmond G, Rizzardini G, Jaeger H, Orrell C, Nagimova F, Bredeek F, García Deltoro M, Swindells S, Andrade-Villanueva JF, et al. . 2020. Long-acting cabotegravir and rilpivirine dosed every 2 months in adults with HIV-1 infection (ATLAS-2M), 48-week results: a randomised, multicentre, open-label, phase 3b, non-inferiority study. The Lancet 396:1994–2005. doi:10.1016/S0140-6736(20)32666-0 - DOI - PubMed
-
- Marzinke MA, Grinztejn B, Fogel JM, Piwowar-Manning E, Li M, Weng L, McCauley M, Cummings V, Ahmed S, Haines CD, et al. . 2021. Characterization of Human Immunodeficiency Virus (HIV) Infection in Cisgender Men and Transgender Women Who Have Sex With Men Receiving Injectable Cabotegravir for HIV Prevention: HPTN 083. J Infect Dis 224:1581–1592. doi:10.1093/infdis/jiab152 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UM1 AI069423/AI/NIAID NIH HHS/United States
- UM1AI068617/HHS | NIH | National Institute of Allergy and Infectious Diseases (NIAID)
- UM1AI068613/HHS | NIH | National Institute of Allergy and Infectious Diseases (NIAID)
- UM1 AI068619/AI/NIAID NIH HHS/United States
- OPP1154174/Bill and Melinda Gates Foundation (GF)
LinkOut - more resources
Full Text Sources
Medical
