

Diagnostic performance of radiologists in distinguishing post-COVID-19 residual abnormalities from interstitial lung abnormalities
- PMID: 39311916
- PMCID: PMC11913901
- DOI: 10.1007/s00330-024-11075-x
Diagnostic performance of radiologists in distinguishing post-COVID-19 residual abnormalities from interstitial lung abnormalities
Abstract
Objective: Distinguishing post-COVID-19 residual abnormalities from interstitial lung abnormalities (ILA) on CT can be challenging if clinical information is limited. This study aimed to evaluate the diagnostic performance of radiologists in distinguishing post-COVID-19 residual abnormalities from ILA.
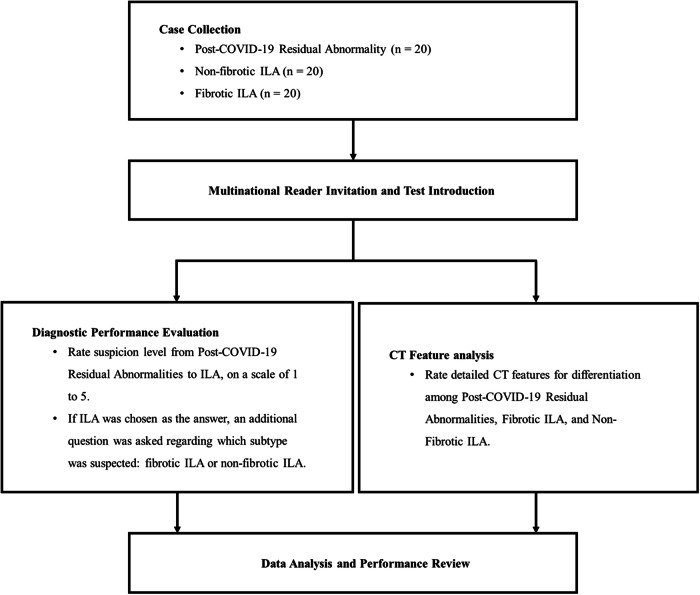
Methods: This multi-reader, multi-case study included 60 age- and sex-matched subjects with chest CT scans. There were 40 cases of ILA (20 fibrotic and 20 non-fibrotic) and 20 cases of post-COVID-19 residual abnormalities. Fifteen radiologists from multiple nations with varying levels of experience independently rated suspicion scores on a 5-point scale to distinguish post-COVID-19 residual abnormalities from fibrotic ILA or non-fibrotic ILA. Interobserver agreement was assessed using the weighted κ value, and the scores of individual readers were compared with the consensus of all readers. Receiver operating characteristic curve analysis was conducted to evaluate the diagnostic performance of suspicion scores for distinguishing post-COVID-19 residual abnormalities from ILA and for differentiating post-COVID-19 residual abnormalities from both fibrotic and non-fibrotic ILA.
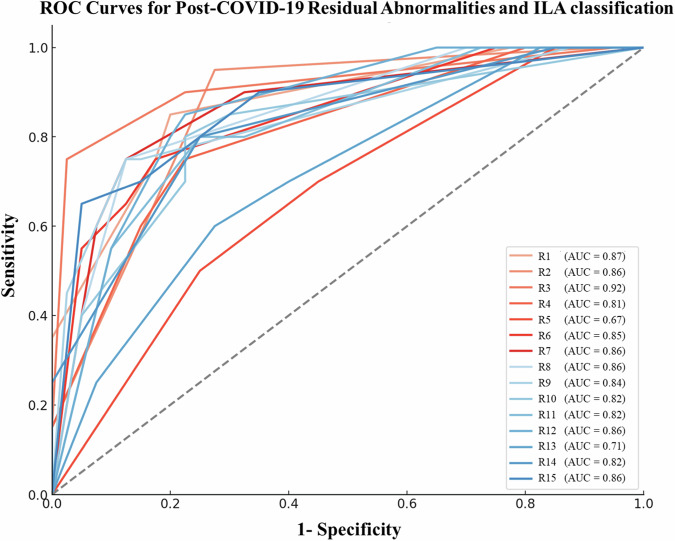
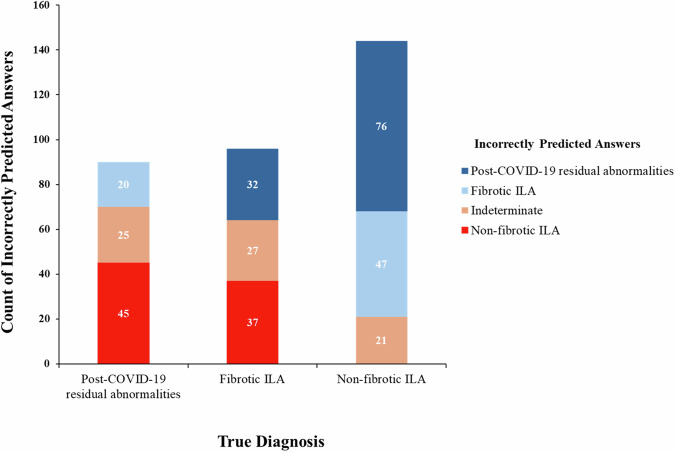
Results: Radiologists' diagnostic performance for distinguishing post-COVID-19 residual abnormalities from ILA was good (area under the receiver operating characteristic curve (AUC) range, 0.67-0.92; median AUC, 0.85) with moderate agreement (κ = 0.56). The diagnostic performance for distinguishing post-COVID-19 residual abnormalities from non-fibrotic ILA was lower than that from fibrotic ILA (median AUC = 0.89 vs. AUC = 0.80, p = 0.003).
Conclusion: Radiologists demonstrated good diagnostic performance and moderate agreement in distinguishing post-COVID-19 residual abnormalities from ILA, but careful attention is needed to avoid misdiagnosing them as non-fibrotic ILA.
Key points: Question How good are radiologists at differentiating interstitial lung abnormalities (ILA) from changes related to COVID-19 infection? Findings Radiologists had a median AUC of 0.85 in distinguishing post-COVID-19 abnormalities from ILA with moderate agreement (κ = 0.56). Clinical relevance Radiologists showed good diagnostic performance and moderate agreement in distinguishing post-COVID-19 residual abnormalities from ILA; nonetheless, caution is needed in distinguishing residual abnormalities from non-fibrotic ILA.
Keywords: COVID-19; Diagnostic imaging; Lung diseases, Interstitial; Tomography, X-ray computed.
© 2024. The Author(s).
Conflict of interest statement
Compliance with ethical standards. Guarantor: The scientific guarantor of this publication is J.E.L. Conflict of interest: H.P. is a deputy editor of European Radiology. They have not participated in the selection nor review processes for this article. S.H.Y. has stocks and stock options in MEDICAL IP. The remaining authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article. Statistics and biometry: No complex statistical methods were necessary for this paper. Informed consent: Written informed consent was waived by the Institutional Review Board. Ethical approval: Institutional Review Board approval was obtained. Study subjects or cohorts overlap: The authors declare that there are no overlapping study subjects or cohorts that have been previously reported in any other study. Methodology: Retrospective Diagnostic study Performed at one institution
Figures
Similar articles
-
Optimizing prone CT use for suspected interstitial lung abnormalities.Eur Radiol. 2025 Jun;35(6):3021-3029. doi: 10.1007/s00330-024-11259-5. Epub 2024 Dec 18. Eur Radiol. 2025. PMID: 39694885 Free PMC article.
-
Interstitial lung abnormalities (ILA) on routine chest CT: Comparison of radiologists' visual evaluation and automated quantification.Eur J Radiol. 2022 Dec;157:110564. doi: 10.1016/j.ejrad.2022.110564. Epub 2022 Oct 17. Eur J Radiol. 2022. PMID: 36308851
-
Effect of contrast enhancement on diagnosis of interstitial lung abnormality in automatic quantitative CT measurement.Eur Radiol. 2025 Jun 3. doi: 10.1007/s00330-025-11715-w. Online ahead of print. Eur Radiol. 2025. PMID: 40459739
-
Interstitial lung abnormalities: prognostic stratification of subtle radiological findings.Curr Opin Pulm Med. 2018 Sep;24(5):432-439. doi: 10.1097/MCP.0000000000000497. Curr Opin Pulm Med. 2018. PMID: 29939864 Review.
-
Interstitial Lung Abnormalities: State of the Art.Radiology. 2021 Oct;301(1):19-34. doi: 10.1148/radiol.2021204367. Epub 2021 Aug 10. Radiology. 2021. PMID: 34374589 Free PMC article. Review.
Cited by
-
Quantification of progressive pulmonary fibrosis by visual scoring of HRCT images: recommendations from Italian chest radiology experts.Radiol Med. 2025 Jun;130(6):965-977. doi: 10.1007/s11547-025-01985-1. Epub 2025 Apr 7. Radiol Med. 2025. PMID: 40192924 Free PMC article. Review.
References
-
- World Health Organization (WHO) COVID-19 dashboard. https://data.who.int/dashboards/covid19/cases/. Accessed March, 2023
-
- Fabbri L, Moss S, Khan FA et al (2023) Parenchymal lung abnormalities following hospitalisation for COVID-19 and viral pneumonitis: a systematic review and meta-analysis. Thorax 78:191–201 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
