

Radiation-emitting metallic stent for unresectable Bismuth type III or IV perihilar cholangiocarcinoma: a multicenter randomized trial
- PMID: 39311927
- PMCID: PMC11745636
- DOI: 10.1097/JS9.0000000000002089
Radiation-emitting metallic stent for unresectable Bismuth type III or IV perihilar cholangiocarcinoma: a multicenter randomized trial
Abstract
Background and aims: Self-expandable metallic stents (SEMSs) have been recommended for patients with unresectable malignant biliary obstruction, while radiation-emitting metallic stents (REMSs) loaded with 125 I seeds have recently been approved to provide longer patency and overall survival in malignant biliary tract obstruction. This trial is to evaluate the efficacy and safety of REMS plus hepatic arterial infusion chemotherapy (REMS-HAIC) versus SEMS plus HAIC (SEMS-HAIC) for unresectable perihilar cholangiocarcinoma (pCCA).
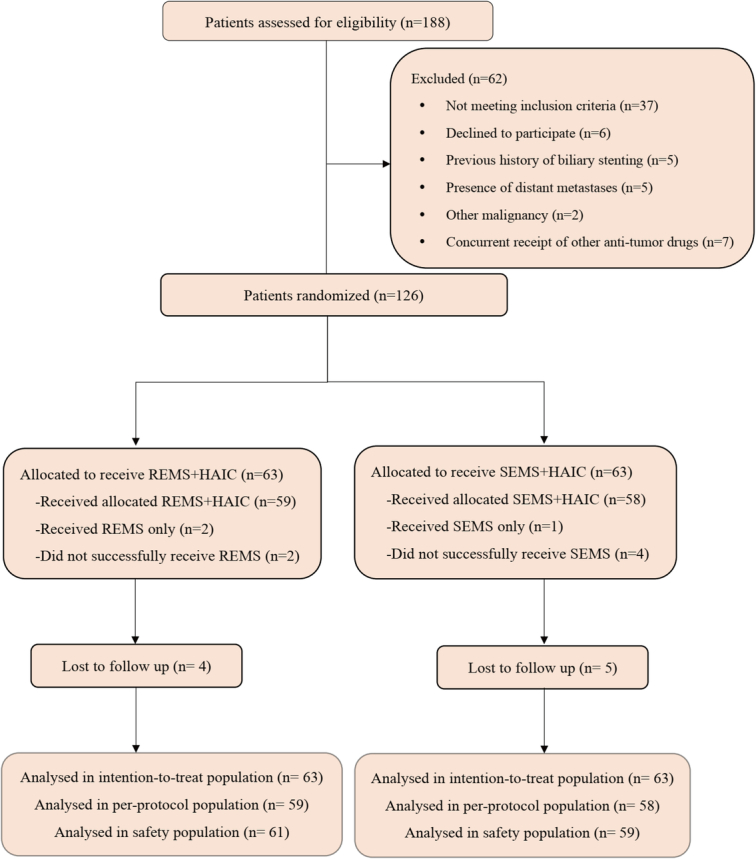
Materials and methods: This multicenter randomized controlled trial recruited patients with unresectable Bismuth type III or IV pCCA between March 2021 and January 2023. Patients were randomly assigned (1:1 ratio) to receive either REMS-HAIC or SEMS-HAIC using permuted block randomization, with a block size of six. The primary endpoint was overall survival (OS). The secondary endpoints were time to symptomatic progression (TTSP), stent patency, relief of jaundice, quality of life, and safety.
Results: A total of 126 patients were included in the intent-to-treat population, with 63 in each group. The median OS was 10.2 months versus 6.7 months ( P =0.002). The median TTSP was 8.6 months versus 5.4 months ( P =0.003). The median stent patency was longer in the REMS-HAIC group than in the SEMS-HAIC group ( P =0.001). The REMS-HAIC group showed better improvement in physical functioning scale ( P <0.05) and fatigue symptoms ( P <0.05) when compared to the SEMS-HAIC group. No significant differences were observed in relief of jaundice (85.7% vs. 84.1%; P =0.803) or the incidence of grade 3 or 4 adverse events (9.8% vs. 11.9%; P =0.721).
Conclusion: REMS plus HAIC showed better OS, TTSP, and stent patency compared with SEMS plus HAIC in patients with unresectable Bismuth type III or IV pCCA with an acceptable safety profile.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no conflicts of interest.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures








References
-
- Vithayathil M, Khan SA. Current epidemiology of cholangiocarcinoma in Western countries. J Hepatol 2022;77:1690–1698. - PubMed
-
- Cadamuro M, Al-Taee A, Gonda TA. Advanced endoscopy meets molecular. diagnosis of cholangiocarcinoma. J Hepatol 2023;78:1063–1072. - PubMed
-
- Roth GS, Neuzillet C, Sarabi M, et al. . Cholangiocarcinoma: what are the options in all comers and how has the advent of molecular profiling opened the way to personalised medicine? Eur J Cancer 2023;179:1–14. - PubMed
-
- Valle JW, Kelley RK, Nervi B, et al. . Biliary tract cancer. Lancet 2021;397:428–444. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
