

Impact of airway closure and lung collapse on inhaled nitric oxide effect in acute lung injury: an experimental study
- PMID: 39312044
- PMCID: PMC11420414
- DOI: 10.1186/s13613-024-01378-z
Impact of airway closure and lung collapse on inhaled nitric oxide effect in acute lung injury: an experimental study
Abstract
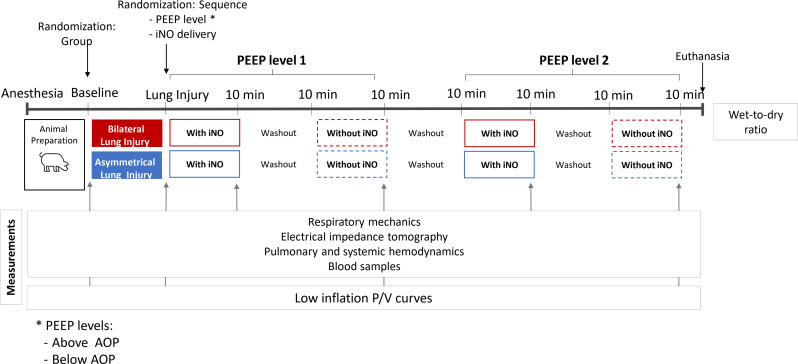
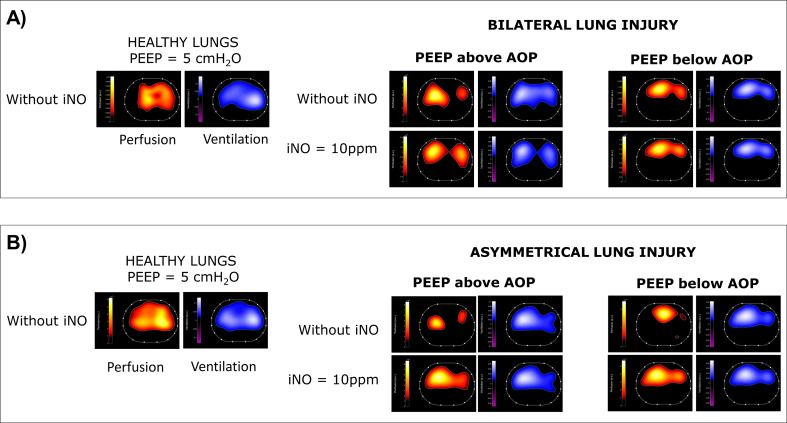
Background: Efficacy of inhaled therapy such as Nitric Oxide (iNO) during mechanical ventilation may depend on airway patency. We hypothesized that airway closure and lung collapse, countered by positive end-expiratory pressure (PEEP), influence iNO efficacy. This could support the role of an adequate PEEP titration for inhalation therapy. The main aim of this study was to assess the effect of iNO with PEEP set above or below the airway opening pressure (AOP) generated by airway closure, on hemodynamics and gas exchange in swine models of acute respiratory distress syndrome. Fourteen pigs randomly underwent either bilateral or asymmetrical two-hit model of lung injury. Airway closure and lung collapse were measured with electrical impedance tomography as well as ventilation/perfusion ratio (V/Q). After AOP detection, the effect of iNO (10ppm) was studied with PEEP set randomly above or below regional AOP. Respiratory mechanics, hemodynamics, and gas-exchange were recorded.
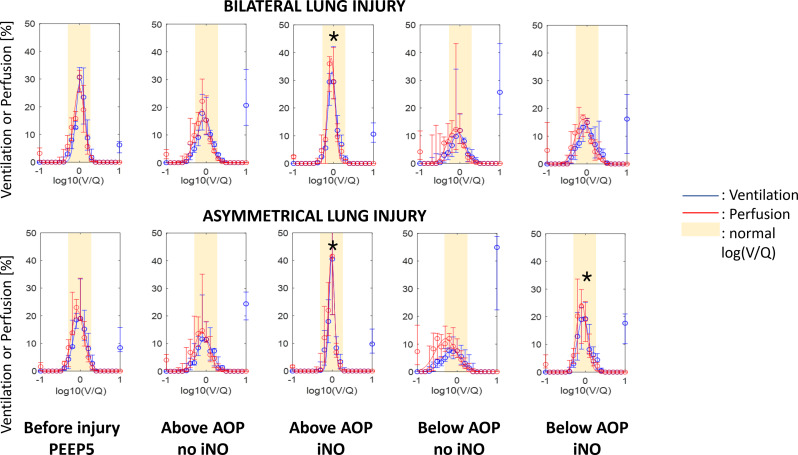
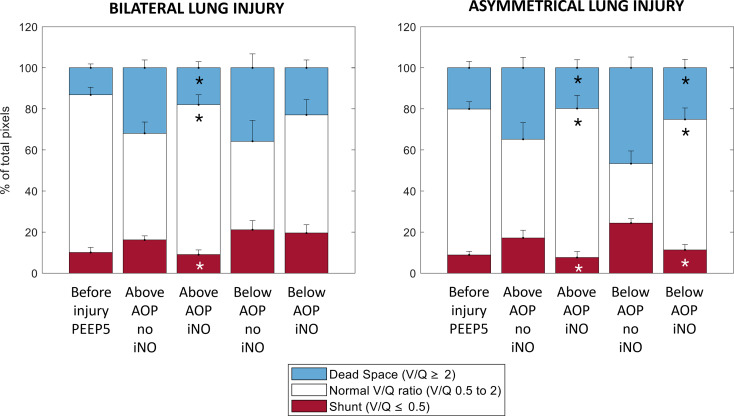
Results: All pigs presented airway closure (AOP > 0.5cmH2O) after injury. In bilateral injury, iNO was associated with an improved mean pulmonary pressure from 49 ± 8 to 42 ± 7mmHg; (p = 0.003), and ventilation/perfusion matching, caused by a reduction in pixels with low V/Q and shunt from 16%[IQR:13-19] to 9%[IQR:4-12] (p = 0.03) only at PEEP set above AOP. iNO had no effect on hemodynamics or gas exchange for PEEP below AOP (low V/Q 25%[IQR:16-30] to 23%[IQR:14-27]; p = 0.68). In asymmetrical injury, iNO improved pulmonary hemodynamics and ventilation/perfusion matching independently from the PEEP set. iNO was associated with improved oxygenation in all cases.
Conclusions: In an animal model of bilateral lung injury, PEEP level relative to AOP markedly influences iNO efficacy on pulmonary hemodynamics and ventilation/perfusion match, independently of oxygenation.
Keywords: (3 to 10) nitric oxide; Acute respiratory distress syndrome; Airway closure; Mechanical ventilation.
© 2024. The Author(s).
Conflict of interest statement
All authors disclose any financial and personal conflicts of interest.
Figures


References
-
- The ARDS Definition Task Force. Acute respiratory distress syndrome: the Berlin definition. JAMA. 2012;307:2526–33. - PubMed
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, et al. Epidemiology, patterns of Care, and mortality for patients with Acute Respiratory Distress Syndrome in Intensive Care Units in 50 countries. JAMA. 2016;315:788–800. - PubMed
-
- Thille AW, Esteban A, Fernández-Segoviano P, Rodriguez J-M, Aramburu J-A, Vargas-Errázuriz P, et al. Chronology of histological lesions in acute respiratory distress syndrome with diffuse alveolar damage: a prospective cohort study of clinical autopsies. Lancet Respir Med. 2013;1:395–401. - PubMed
-
- Zapol WM, Jones R. Vascular components of ARDS: clinical pulmonary hemodynamics and morphology. Am Rev Respir Dis. 1987;136:471–4. - PubMed
LinkOut - more resources
Full Text Sources
