

Posthospitalization COVID-19 cognitive deficits at 1 year are global and associated with elevated brain injury markers and gray matter volume reduction
- PMID: 39312956
- PMCID: PMC11750706
- DOI: 10.1038/s41591-024-03309-8
Posthospitalization COVID-19 cognitive deficits at 1 year are global and associated with elevated brain injury markers and gray matter volume reduction
Abstract
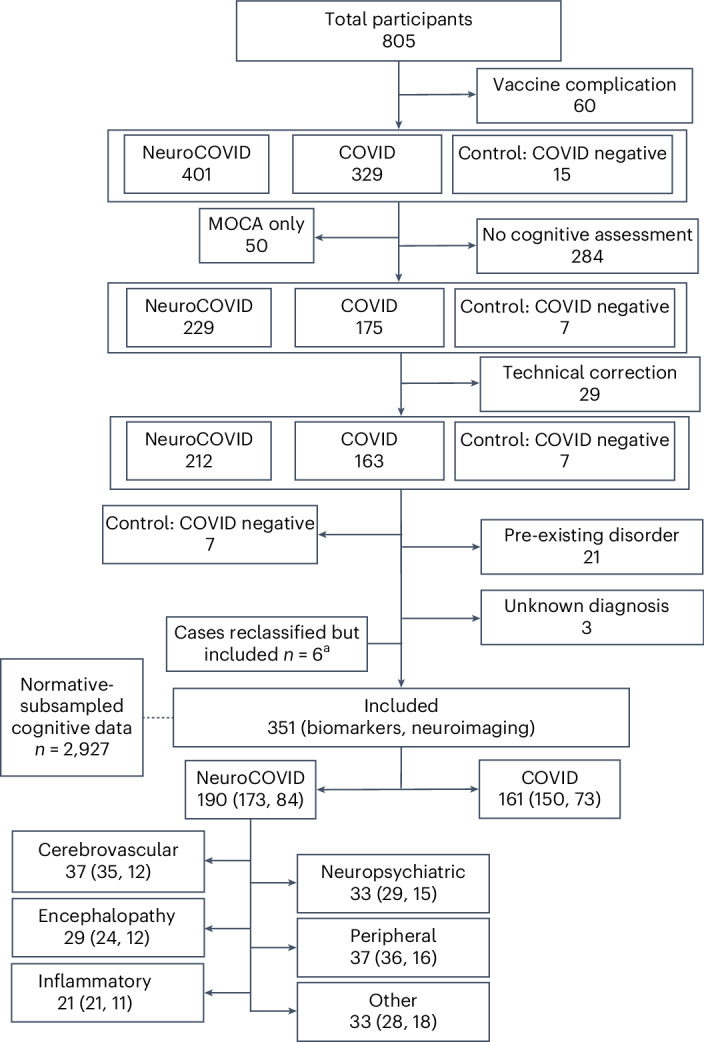
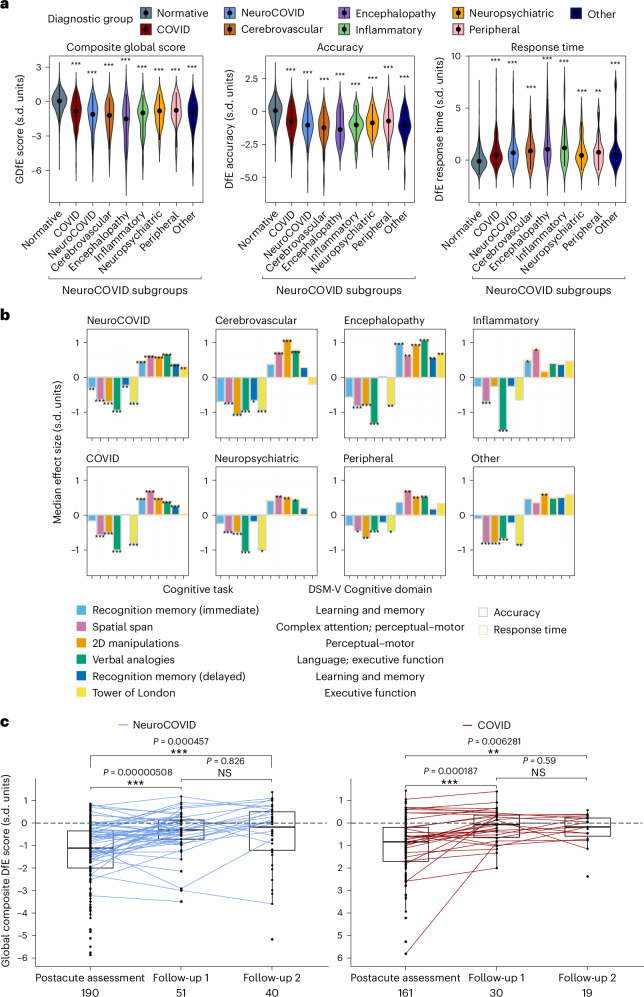
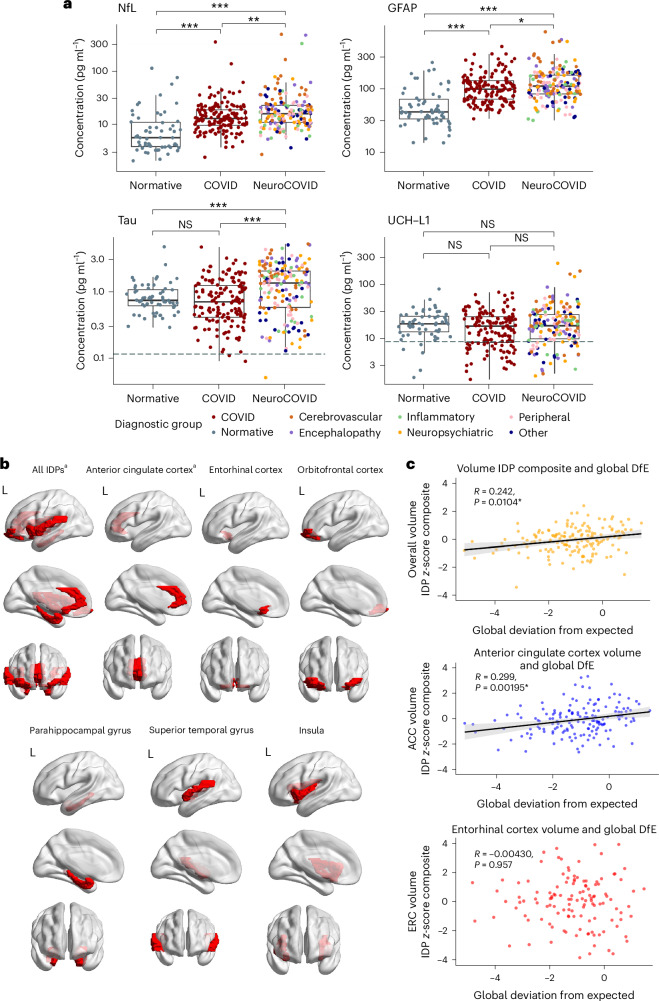
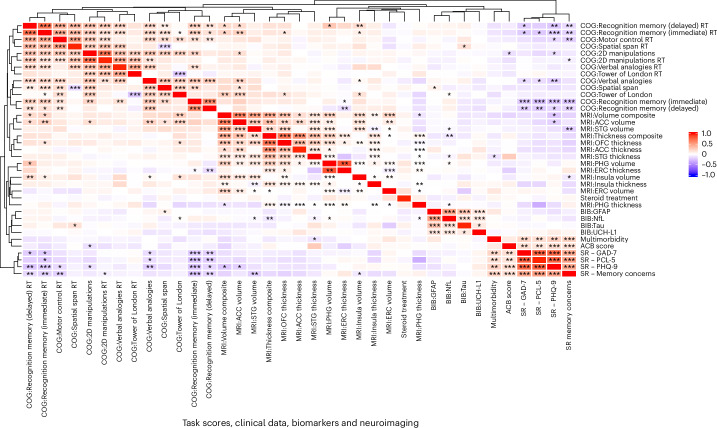
The spectrum, pathophysiology and recovery trajectory of persistent post-COVID-19 cognitive deficits are unknown, limiting our ability to develop prevention and treatment strategies. We report the 1-year cognitive, serum biomarker and neuroimaging findings from a prospective, national study of cognition in 351 COVID-19 patients who required hospitalization, compared with 2,927 normative matched controls. Cognitive deficits were global, associated with elevated brain injury markers and reduced anterior cingulate cortex volume 1 year after COVID-19. Severity of the initial infective insult, postacute psychiatric symptoms and a history of encephalopathy were associated with the greatest deficits. There was strong concordance between subjective and objective cognitive deficits. Longitudinal follow-up in 106 patients demonstrated a trend toward recovery. Together, these findings support the hypothesis that brain injury in moderate to severe COVID-19 may be immune-mediated, and should guide the development of therapeutic strategies.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: R.A.I.B. holds equity and serves as a director for Centile Bioscience Inc. P.J.H. holds equity and serves as director for H2 Cognitive Designs LTD. R.U. was speaker at a promotional educational event for Otuska; and reports consultancy for Vitaris and Springer Healthcare in the past 3 years. T.A.P. reports consultancy for Arialys Therapeutics Inc. and speaker honoraria from Janssen. A.C. is President of the FND Society, Associate Editor of JNNP, and gives independent testimony in court on a range of neuropsychiatric topics. E.B. consults for GSK, SR One, Boehringer Ingelheim and Sosei Heptares. T.S. is Director of The Pandemic Institute, which has received funding from Innova and CSL Seqirus, and Aviva and DAM Health. T.S. was an advisor to the GSK Ebola Vaccine program and the Siemens Diagnostic Program. T.S. chaired the Siemens Healthineers Clinical Advisory Board. T.S. co-chaired the WHO Neuro-COVID task force and sat on the UK Government Advisory Committee on Dangerous Pathogens, and the Medicines and Healthcare Products Regulatory Agency (MHRA) Expert Working Group on COVID-19 vaccines. T.S. advised to the UK COVID-19 Therapeutics Advisory Panel. T.S. was a member of the COVID-19 Vaccines Benefit Risk Expert Working Group for the Commission on Human Medicines committee of the MHRA. T.S. has been a member of the Encephalitis Society since 1998 and President of the Encephalitis Society since 2019. The remaining authors declare no competing interests.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
