

Successful Interventional Therapy for Portal Vein Stenosis after Ex Vivo Liver Resection and Autotransplantation in End-Stage Hepatic Alveolar Echinococcosis with Cavernous Transformation
- PMID: 39313918
- PMCID: PMC11438022
- DOI: 10.12659/AOT.944851
Successful Interventional Therapy for Portal Vein Stenosis after Ex Vivo Liver Resection and Autotransplantation in End-Stage Hepatic Alveolar Echinococcosis with Cavernous Transformation
Abstract
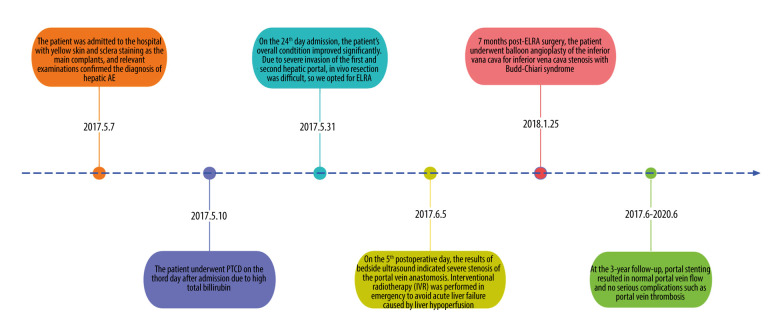
BACKGROUND End-stage hepatic alveolar echinococcosis (AE) can result in cavernous transformation of the portal vein (CTPV) due to extensive invasion of the portal vein. Ex vivo liver resection and autotransplantation (ELRA) is a new treatment option for patients with end-stage hepatic AE combined with CTPV. ELRA can achieve radical resection of HAE lesions and vascular reconstruction, and also effectively controls bleeding, particularly in cases involving multiple tortuous PV collaterals. Unfortunately, postoperative complications related to the portal vein can impede liver blood flow, thereby increasing the risk of portal hypertension and eventual failure of the transplanted liver if not promptly treated through appropriate medical interventions. CASE REPORT We report the case of a 31-year-old woman who underwent ELRA for end-stage hepatic AE combined with CTPV, and early postoperative portal vein anastomotic stenosis occurred. Stenting of the portal vein was performed after clarification of the stenotic segment by portal venography, followed by anticoagulation therapy and close ultrasound follow-up. After the operation, the patient's portal vein anastomosis widened and the blood flow into the liver returned to normal, avoiding graft liver failure. At 3-year follow-up, the portal vein stent was patent and no serious portal vein complications such as thrombosis had occurred. CONCLUSIONS ELRA provides a new therapeutic approach for patients with HAE combined with CTPV, and intraoperative portal vein reconstruction is one of the key procedures. For CTPV patients with early postoperative portal vein stenosis, interventional therapy (IVR) offers fresh perspectives and avoids acute liver failure caused by liver hypoperfusion.
Conflict of interest statement
Figures



Similar articles
-
Application of ex vivo liver resection and autotransplantation in treating Budd-Chiari syndrome secondary to end-stage hepatic alveolar echinococcosis: A case series.Medicine (Baltimore). 2021 Aug 27;100(34):e27075. doi: 10.1097/MD.0000000000027075. Medicine (Baltimore). 2021. PMID: 34449508 Free PMC article.
-
Treatment of Cavernous Transformation of Portal Vein Caused by Hepatic Cystic Echinococcosis Using Ex Vivo Liver Resection and Autotransplantation.Ann Transplant. 2024 Apr 16;29:e942358. doi: 10.12659/AOT.942358. Ann Transplant. 2024. PMID: 38622855 Free PMC article.
-
Vascular infiltration-based surgical planning in treating end-stage hepatic alveolar echinococcosis with ex vivo liver resection and autotransplantation.Surgery. 2019 May;165(5):889-896. doi: 10.1016/j.surg.2018.11.007. Epub 2018 Dec 24. Surgery. 2019. PMID: 30591376
-
Massive sympathetic nerve infiltration in advanced hepatic alveolar echinococcosis: a case report and review of the literature.BMC Infect Dis. 2022 May 23;22(1):489. doi: 10.1186/s12879-022-07470-8. BMC Infect Dis. 2022. PMID: 35606711 Free PMC article. Review.
-
Living donor liver transplantation for idiopathic portal hypertension with extrahepatic portal vein stenosis and splenic artery aneurysms: a case report and review of the literature.BMC Surg. 2020 Oct 29;20(1):257. doi: 10.1186/s12893-020-00921-6. BMC Surg. 2020. PMID: 33121468 Free PMC article. Review.
Cited by
-
Endovascular Intervention of Portal Vein Stenosis in Pediatric Patients After Liver Transplantation: A Single-Center Experience.Ann Transplant. 2025 Aug 19;30:e949532. doi: 10.12659/AOT.949532. Ann Transplant. 2025. PMID: 40826828 Free PMC article.
-
Ex vivo Liver Autotransplantation for Alveolar Echinococcosis with Brain and Lung Metastases: A Case Report.Int Med Case Rep J. 2025 Apr 5;18:473-478. doi: 10.2147/IMCRJ.S507833. eCollection 2025. Int Med Case Rep J. 2025. PMID: 40206270 Free PMC article.
References
-
- Brunetti E, Kern P, Vuitton DA Writing Panel for the WHO-IWGE. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 2010;114(1):1–16. - PubMed
-
- Thomas MN, Zwingelberg S, Angele M, et al. [Diagnosis and treatment of cystic and alveolar echinococcosis]. MMW Fortschr Med. 2017;159(14):38–42. [in German] - PubMed
-
- Hwang R, Liou P, Kato T. Ex vivo liver resection and autotransplantation: An emerging option in selected indications. JJ Hepatol. 2018;69(5):1002–3. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
