

This is a preprint.
Robust Real-time Segmentation of Bio-Morphological Features in Human Cherenkov Imaging during Radiotherapy via Deep Learning
- PMID: 39314506
- PMCID: PMC11419192
Robust Real-time Segmentation of Bio-Morphological Features in Human Cherenkov Imaging during Radiotherapy via Deep Learning
Update in
-
Robust real-time segmentation of bio-morphological features in human cherenkov imaging during radiotherapy via deep learning.Med Phys. 2025 Aug;52(8):e18002. doi: 10.1002/mp.18002. Med Phys. 2025. PMID: 40781822
Abstract
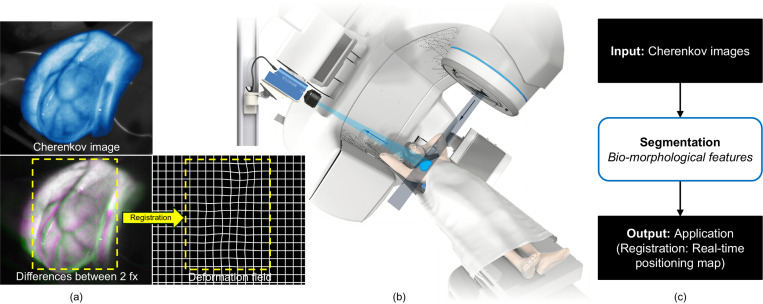
Cherenkov imaging enables real-time visualization of megavoltage X-ray or electron beam delivery to the patient during Radiation Therapy (RT). Bio-morphological features, such as vasculature, seen in these images are patient-specific signatures that can be used for verification of positioning and motion management that are essential to precise RT treatment. However until now, no concerted analysis of this biological feature-based tracking was utilized because of the slow speed and accuracy of conventional image processing for feature segmentation. This study demonstrated the first deep learning framework for such an application, achieving video frame rate processing. To address the challenge of limited annotation of these features in Cherenkov images, a transfer learning strategy was applied. A fundus photography dataset including 20,529 patch retina images with ground-truth vessel annotation was used to pre-train a ResNet segmentation framework. Subsequently, a small Cherenkov dataset (1,483 images from 212 treatment fractions of 19 breast cancer patients) with known annotated vasculature masks was used to fine-tune the model for accurate segmentation prediction. This deep learning framework achieved consistent and rapid segmentation of Cherenkov-imaged bio-morphological features on another 19 patients, including subcutaneous veins, scars, and pigmented skin. Average segmentation by the model achieved Dice score of 0.85 and required less than 0.7 milliseconds processing time per instance. The model demonstrated outstanding consistency against input image variances and speed compared to conventional manual segmentation methods, laying the foundation for online segmentation in real-time monitoring in a prospective setting.
Keywords: Cherenkov imaging; Image segmentation; Morphological feature; Radiotherapy; Transfer learning.
Figures






References
-
- Bogdanich W., “Radiation Offers New Cures, and Ways to Do Harm,” The New York Times, Jan. 23, 2010. Accessed: Nov. 13, 2023. [Online]. Available: https://www.nytimes.com/2010/01/24/health/24radiation.html
-
- Jarvis L. A. et al. , “Initial Clinical Experience of Cherenkov Imaging in External Beam Radiation Therapy Identifies Opportunities to Improve Treatment Delivery,” International Journal of Radiation Oncology*Biology*Physics, vol. 109, no. 5, pp. 1627–1637, Apr. 2021, doi: 10.1016/j.ijrobp.2020.11.013. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources