

Exploring the Spectrum of Electrolyte Imbalances in Preeclampsia: Mechanisms, Implications, and Clinical Insights
- PMID: 39314616
- PMCID: PMC11418792
- DOI: 10.7759/cureus.67666
Exploring the Spectrum of Electrolyte Imbalances in Preeclampsia: Mechanisms, Implications, and Clinical Insights
Abstract
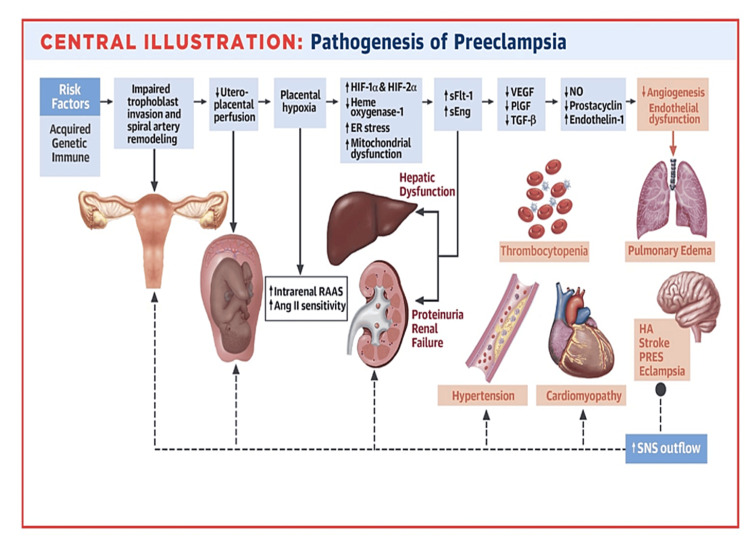
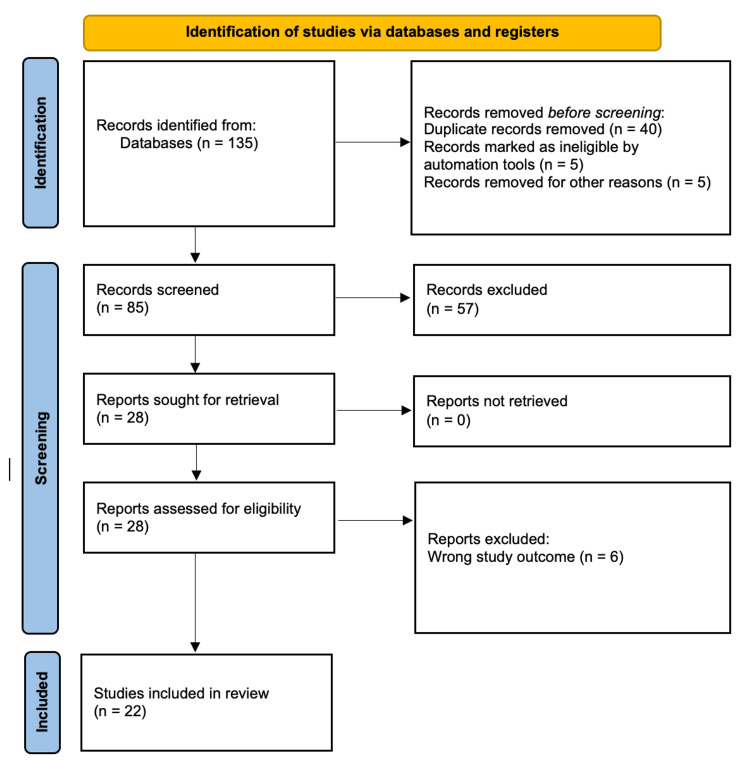
Preeclampsia, a complex and perplexing disorder unique to pregnancy, is widely recognized as primarily originating from placental dysfunction and can only be resolved by the delivery of the fetus in severe cases. Preeclampsia is a prevalent medical issue during pregnancy and is associated with elevated rates of maternal and infant mortality and morbidity. The exact cause of preeclampsia remains uncertain, although multiple factors have been implicated in its development based on current knowledge. Preeclampsia is characterized by maternal endothelial dysfunction due to the presence of fetal-derived circulatory substances from the placenta. The condition is associated with various risk factors, including maternal comorbidities such as chronic renal disease, hypertension (HTN), and obesity. Additionally, a family history of preeclampsia, nulliparity, multiple gestations, previous instances of preeclampsia, or intrauterine fetal growth restriction (IUGR) are considered risk factors. Electrolytes, including sodium, potassium, and chloride, play a critical role in the function of vascular smooth muscles and may potentially contribute to the pathophysiology of hypertension. In this review, we have summarized the literature on electrolytes in preeclampsia by conducting an extensive systematic search of databases such as PubMed, Excerpta Medica database (EMBASE), and Medical Literature Analysis and Retrieval System Online (MEDLINE).
Keywords: derangement; electrolyte; gestational hypertension; preeclampsia; pregnancy-induced hypertension.
Copyright © 2024, Gupta et al.
Conflict of interest statement
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Management of preeclampsia.Pregnancy Hypertens. 2014 Jul;4(3):246-7. doi: 10.1016/j.preghy.2014.04.021. Epub 2014 Jul 9. Pregnancy Hypertens. 2014. PMID: 26104648
-
An integrated model of preeclampsia: a multifaceted syndrome of the maternal cardiovascular-placental-fetal array.Am J Obstet Gynecol. 2022 Feb;226(2S):S963-S972. doi: 10.1016/j.ajog.2020.10.023. Epub 2021 Mar 9. Am J Obstet Gynecol. 2022. PMID: 33712272 Review.
-
Preeclampsia: Recent Advances in Predicting, Preventing, and Managing the Maternal and Fetal Life-Threatening Condition.Int J Environ Res Public Health. 2023 Feb 8;20(4):2994. doi: 10.3390/ijerph20042994. Int J Environ Res Public Health. 2023. PMID: 36833689 Free PMC article. Review.
-
Preeclampsia, gestational hypertension and intrauterine growth restriction, related or independent conditions?Am J Obstet Gynecol. 2006 Apr;194(4):921-31. doi: 10.1016/j.ajog.2005.10.813. Am J Obstet Gynecol. 2006. PMID: 16580277
-
Using ultrasound and angiogenic markers from a 19- to 23-week assessment to inform the subsequent diagnosis of preeclampsia.Am J Obstet Gynecol. 2022 Aug;227(2):294.e1-294.e11. doi: 10.1016/j.ajog.2022.03.007. Epub 2022 Mar 9. Am J Obstet Gynecol. 2022. PMID: 35276067
Cited by
-
Hematological and biochemical alterations in preeclampsia: Readings from cord blood analysis.PLoS One. 2025 May 30;20(5):e0324460. doi: 10.1371/journal.pone.0324460. eCollection 2025. PLoS One. 2025. PMID: 40446190 Free PMC article.
References
-
- Preeclampsia: disease biology and burden, its management strategies with reference to India. Malik A, Jee B, Gupta SK. Pregnancy Hypertens. 2019;15:23–31. - PubMed
-
- The role of calcium, magnesium, and zinc in pre-eclampsia. Jain S, Sharma P, Kulshreshtha S, Mohan G, Singh S. Biol Trace Elem Res. 2010;133:162–170. - PubMed
-
- Hypoxia-reoxygenation: a potent inducer of apoptotic changes in the human placenta and possible etiological factor in preeclampsia. Hung TH, Skepper JN, Charnock-Jones DS, Burton GJ. Circ Res. 2002;90:1274–1281. - PubMed
Publication types
LinkOut - more resources
Full Text Sources