

Unusual presentation of a splenic infarction
- PMID: 39314663
- PMCID: PMC11418093
- DOI: 10.1016/j.radcr.2024.08.124
Unusual presentation of a splenic infarction
Abstract
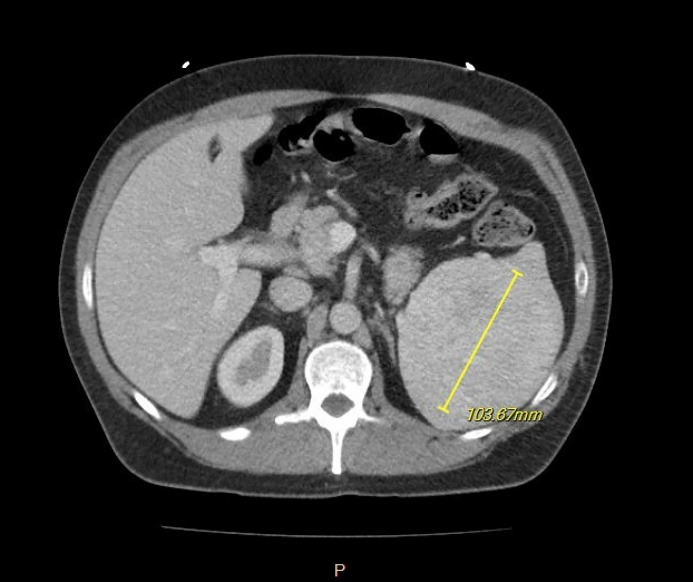
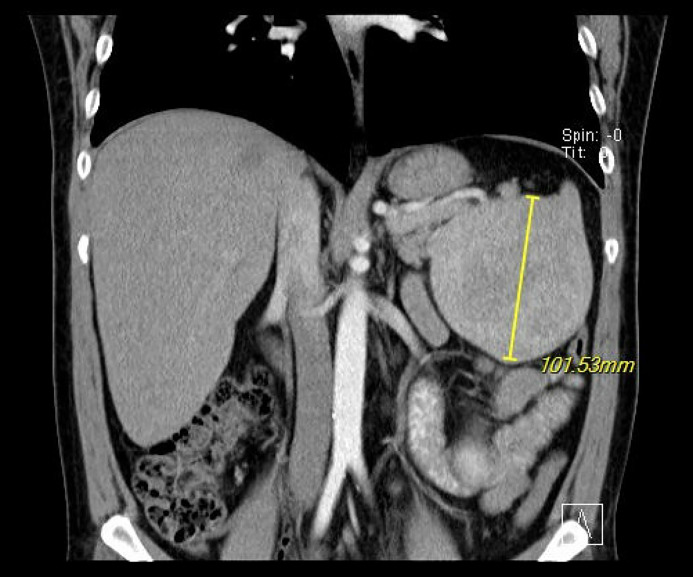
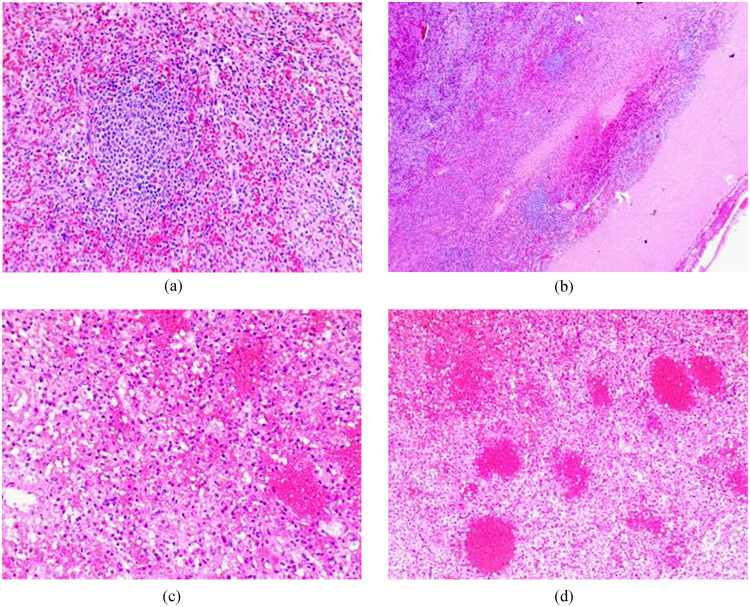
A 41-year-old male with a history of tobacco and alcohol use presented to our clinic for a follow up of an incidentally diagnosed splenic mass. The patient was sent for further diagnostic evaluation, and computed tomography showed a large splenic mass with heterogenous enhancement raising concern for neoplasm. Due to the uncertain nature of the splenic lesion and high complication rate of percutaneous splenic biopsy, a splenectomy was performed. The specimen was sent to pathology, and the report favored neoplasm but was inconclusive. The samples were sent to another institution for a consult, where the patient's spleen was determined to be the result of a previously suffered hemorrhagic infarct. This case demonstrates the difficulty of diagnosing splenic lesions using diagnostic imaging and the discrepancy that may occur between radiology and pathology assessments. In the setting of uncertain pathology, the removal of what might be a functional spleen is often preferred over a percutaneous biopsy due to concerns of intraabdominal bleeding and tumor dissemination.
Keywords: Case report; Splenectomy; Splenic infarction; Splenic lesion; Splenic neoplasm.
© 2024 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
