

This is a preprint.
Antibiotic De-escalation Patterns and Outcomes in Critically Ill Patients with Suspected Pneumonia as Informed by Bronchoalveolar Lavage Results
- PMID: 39314979
- PMCID: PMC11419224
- DOI: 10.1101/2024.09.10.24313149
Antibiotic De-escalation Patterns and Outcomes in Critically Ill Patients with Suspected Pneumonia as Informed by Bronchoalveolar Lavage Results
Update in
-
Antibiotic de-escalation patterns and outcomes in critically ill patients with suspected pneumonia as informed by bronchoalveolar lavage results.Eur J Clin Microbiol Infect Dis. 2025 Aug;44(8):1861-1871. doi: 10.1007/s10096-025-05144-2. Epub 2025 May 3. Eur J Clin Microbiol Infect Dis. 2025. PMID: 40316844 Free PMC article.
Abstract
Background: Antibiotic stewardship in critically ill pneumonia patients is crucial yet challenging, partly due to the limited diagnostic yield of noninvasive infectious tests. In this study, we report an antibiotic prescription pattern informed by bronchoalveolar lavage (BAL) results, where clinicians de-escalate antibiotics based on the combination of quantitative cultures and multiplex PCR rapid diagnostic tests.
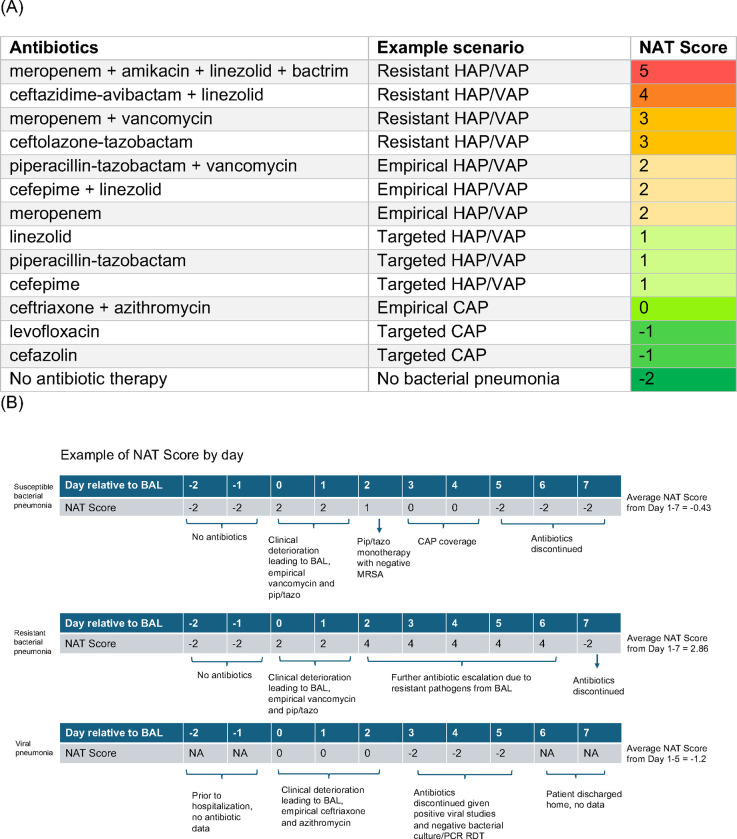
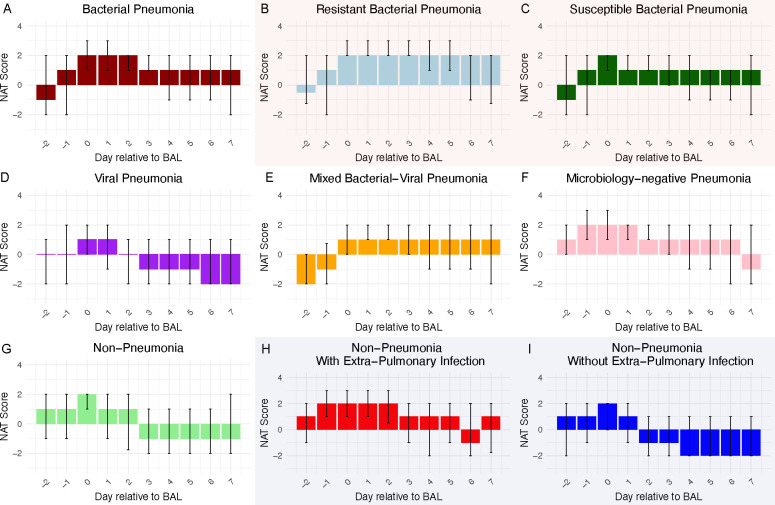
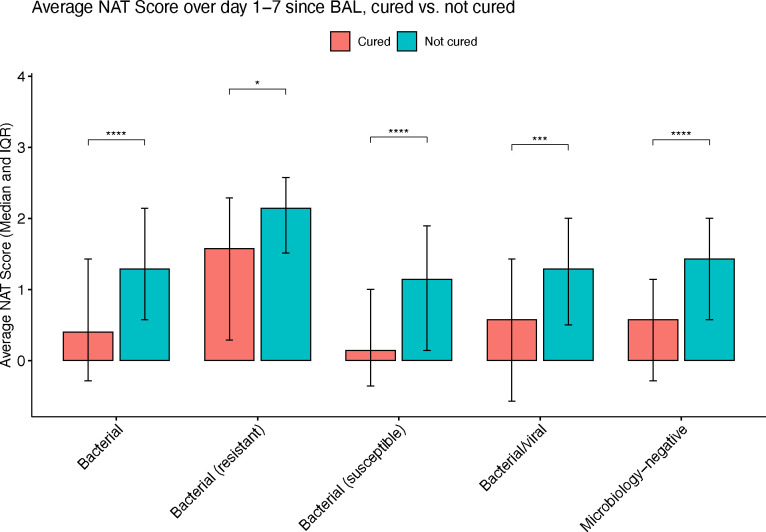
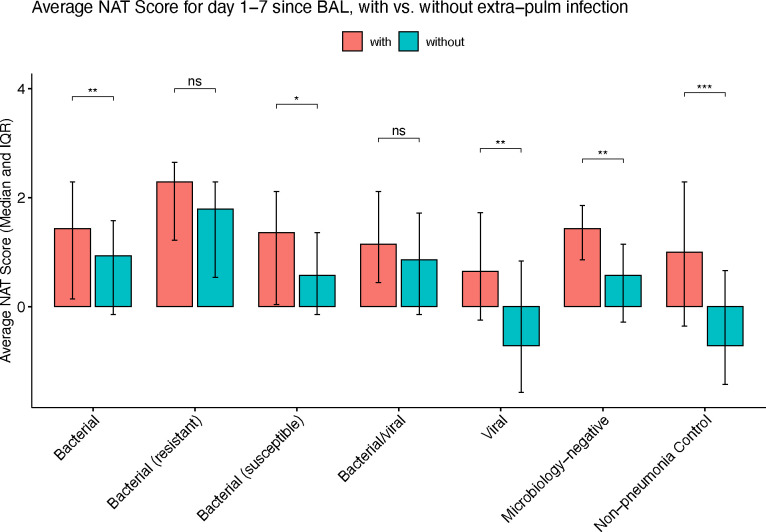
Methods: We analyzed data from SCRIPT, a single-center prospective cohort study of mechanically ventilated patients who underwent a BAL for suspected pneumonia. We used the novel Narrow Antibiotic Therapy (NAT) score to quantify day-by-day antibiotic prescription pattern for each suspected pneumonia episode etiology (bacterial, viral, mixed bacterial/viral, microbiology-negative, and non-pneumonia control). We also analyzed and compared clinical outcomes for each pneumonia etiology, including unfavorable outcomes (a composite of in-hospital mortality, discharge to hospice, or requiring lung transplantation during hospitalization), duration of ICU stay, and duration of intubation. Clinical outcomes were compared with the Mann-Whitney U test and Fisher's exact test.
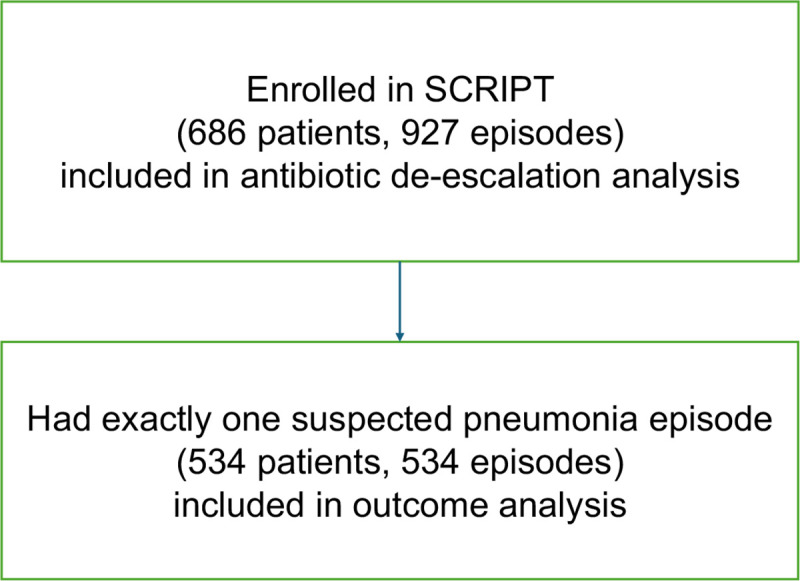
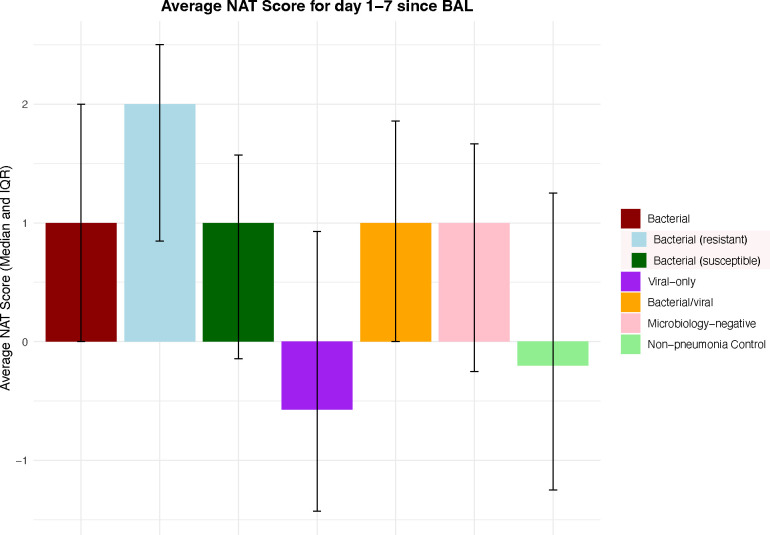
Results: We included 686 patients with 927 pneumonia episodes. NAT score analysis indicated that an antibiotic de-escalation pattern was evident in all pneumonia etiologies except resistant bacterial pneumonia. Microbiology-negative pneumonia was treated similarly to susceptible bacterial pneumonia in terms of antibiotic spectrum. Over a quarter of the time in viral pneumonia episodes, antibiotics were completely discontinued. Unfavorable outcomes were comparable across all pneumonia etiologies. Patients with viral and mixed bacterial/viral pneumonia had longer durations of ICU stay and intubation.
Conclusions: BAL quantitative cultures and multiplex PCR rapid diagnostic tests resulted in prompt antibiotic de-escalation in critically ill pneumonia patients. There was no evidence of increased incidence of unfavorable outcomes.
Conflict of interest statement
Declarations of interests: BDS holds US patent 10,905,706, “Compositions and methods to accelerate resolution of acute lung inflammation,” and serves on the scientific advisory board of Zoe Biosciences, in which he holds stock options. Other authors declare no conflicts of interest.
Figures
Similar articles
-
Antibiotic de-escalation patterns and outcomes in critically ill patients with suspected pneumonia as informed by bronchoalveolar lavage results.Eur J Clin Microbiol Infect Dis. 2025 Aug;44(8):1861-1871. doi: 10.1007/s10096-025-05144-2. Epub 2025 May 3. Eur J Clin Microbiol Infect Dis. 2025. PMID: 40316844 Free PMC article.
-
Antibiotics for ventilator-associated pneumonia.Cochrane Database Syst Rev. 2016 Oct 20;10(10):CD004267. doi: 10.1002/14651858.CD004267.pub4. Cochrane Database Syst Rev. 2016. PMID: 27763732 Free PMC article.
-
Short-course versus prolonged-course antibiotic therapy for hospital-acquired pneumonia in critically ill adults.Cochrane Database Syst Rev. 2015 Aug 24;2015(8):CD007577. doi: 10.1002/14651858.CD007577.pub3. Cochrane Database Syst Rev. 2015. PMID: 26301604 Free PMC article.
-
Intracavity lavage and wound irrigation for prevention of surgical site infection.Cochrane Database Syst Rev. 2017 Oct 30;10(10):CD012234. doi: 10.1002/14651858.CD012234.pub2. Cochrane Database Syst Rev. 2017. PMID: 29083473 Free PMC article.
-
Interventions to improve antibiotic prescribing practices for hospital inpatients.Cochrane Database Syst Rev. 2013 Apr 30;(4):CD003543. doi: 10.1002/14651858.CD003543.pub3. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2017 Feb 09;2:CD003543. doi: 10.1002/14651858.CD003543.pub4. PMID: 23633313 Updated.
References
-
- World Health Organization. The Top 10 Causes of Death.
-
- Wunderink RG, Srinivasan A, Barie PS, et al. Antibiotic stewardship in the intensive care unit : An official American thoracic society workshop report in collaboration with the aacn, chest, cdc, and sccm. Ann Am Thorac Soc. 2020;17(5):531–540. doi: 10.1513/AnnalsATS.202003-188ST - DOI - PMC - PubMed
-
- Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63(5):e61–e111. doi: 10.1093/cid/ciw353 - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources