

Sex-specific differences in alive hospital discharge following infrarenal abdominal aortic aneurysm repair
- PMID: 39315612
- PMCID: PMC12055232
- DOI: 10.1093/eurheartj/ehae675
Sex-specific differences in alive hospital discharge following infrarenal abdominal aortic aneurysm repair
Abstract
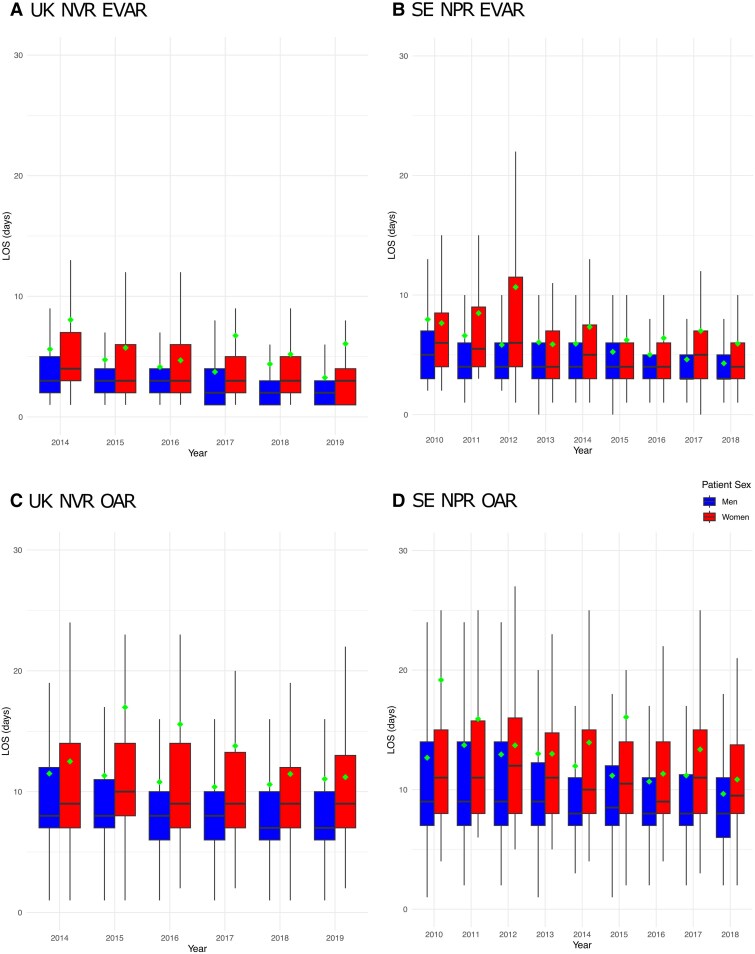
Background and aims: A longer time to alive hospital discharge following infrarenal abdominal aortic aneurysm (AAA) repair is associated with reduced patient satisfaction and increased length of stay, hospital-acquired deconditioning, infection, and costs. This study investigated sex-specific differences in, and drivers of, the rate of alive hospital discharge.
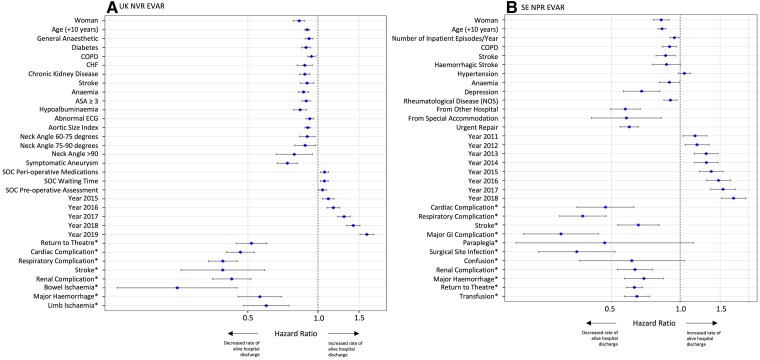
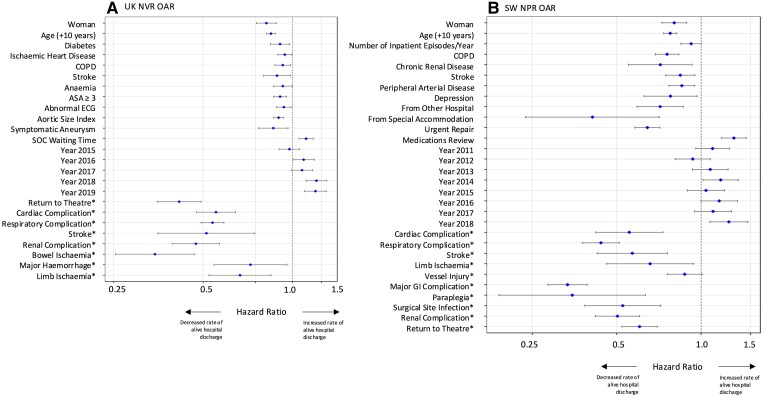
Methods: Examination of UK National Vascular Registry (UK NVR), 2014-19, and Swedish National Patient Registry (SE NPR) elective AAA patients, 2010-18, for endovascular (EVAR) or open aneurysm repair (OAR). Cox models assessed sex-specific difference in the rate of alive hospital discharge, adjusting for co-morbidity, anatomy, standard of care, post-operative complications, and year, with in-hospital death as the competing risk.
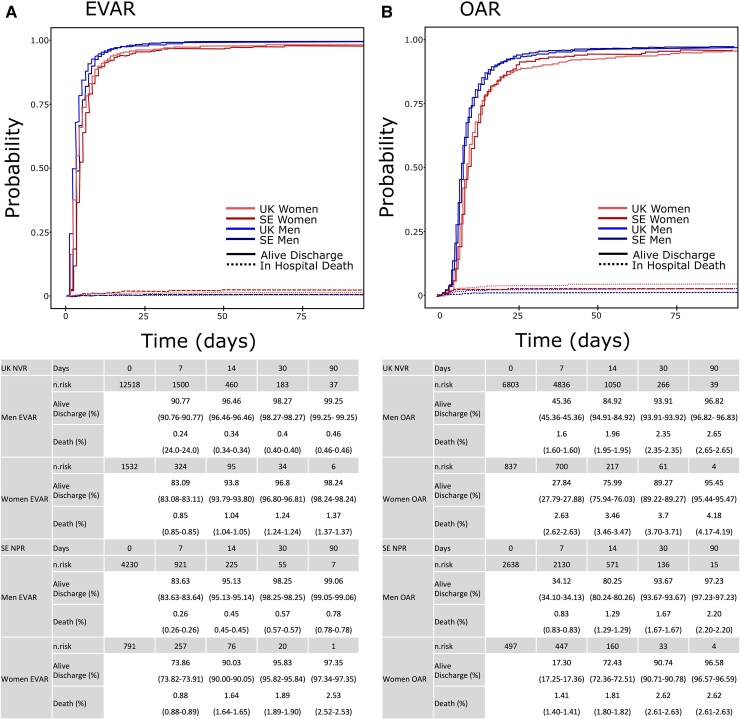
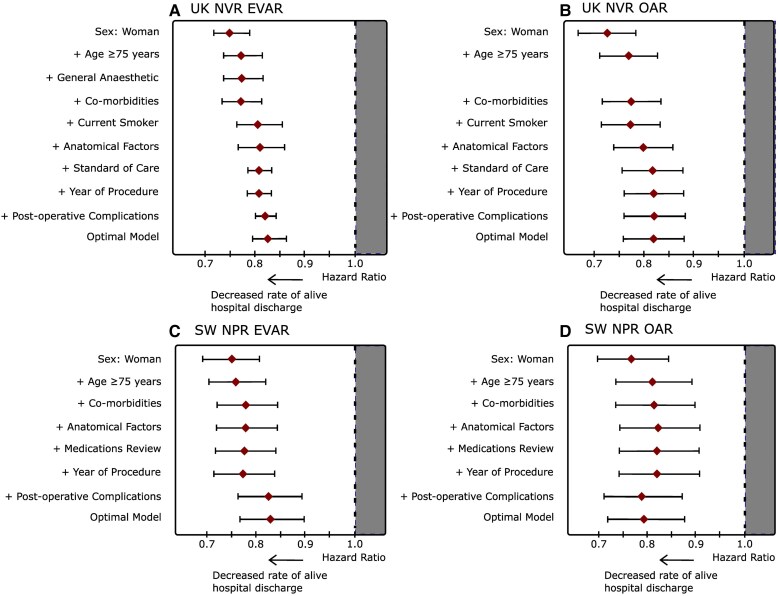
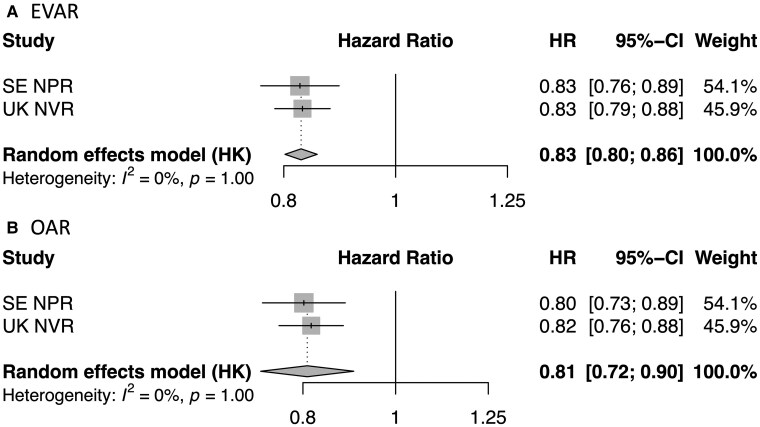
Results: A total of 29 751 AAA repairs (UK NVR: EVAR 12 518:1532; OAR 6803:837; SE NPR: EVAR 4234:792; OAR 2638:497, men:women) were assessed. For EVAR, the unadjusted rate of alive hospital discharge was ∼25% lower for women [UK NVR: hazard ratio (HR) 0.75 (0.71-0.80), P < .001; SE NPR: HR 0.75 (0.69-0.81), P < .001]. Following adjustment, the sex-specific HR narrowed but remained significant [UK NVR: HR 0.83 (0.79-0.88), P < .001; SE NPR: HR 0.83 (0.76-0.89), P < .001]. For OAR, the rate of alive hospital discharge was 23%-27% lower for women [UK NVR: HR 0.73 (0.67-0.78), P < .001; SE NPR: HR 0.77 (0.70-0.85), P < .001]. Following adjustment, the sex-specific HR narrowed [UK NVR: HR 0.82 (0.76-0.88), P < .001; SE NPR: HR 0.79 (0.72-0.88), P < .001] but remained significant.
Conclusions: Women have a 25% lower rate of alive discharge after aortic surgery, despite adjustment for pre/peri- and post-operative parameters. Efforts to increase the rate of alive hospital discharge for women should be sought.
Keywords: Abdominal aortic aneurysm; Length of stay; Sex.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures

Similar articles
-
Sex differences in mortality after abdominal aortic aneurysm repair in the UK.Br J Surg. 2017 Nov;104(12):1656-1664. doi: 10.1002/bjs.10600. Epub 2017 Jul 26. Br J Surg. 2017. PMID: 28745403 Free PMC article.
-
Editor's Choice - Systematic Review and Meta-Analysis of Sex Specific Differences in Adverse Events After Open and Endovascular Intact Abdominal Aortic Aneurysm Repair: Consistently Worse Outcomes for Women.Eur J Vasc Endovasc Surg. 2021 Sep;62(3):367-378. doi: 10.1016/j.ejvs.2021.05.029. Epub 2021 Jul 28. Eur J Vasc Endovasc Surg. 2021. PMID: 34332836
-
Interaction between frailty and sex on mortality after elective abdominal aortic aneurysm repair.J Vasc Surg. 2019 Dec;70(6):1831-1843. doi: 10.1016/j.jvs.2019.01.086. Epub 2019 May 27. J Vasc Surg. 2019. PMID: 31147120 Free PMC article.
-
Gender differences in abdominal aortic aneurysm presentation, repair, and mortality in the Vascular Study Group of New England.J Vasc Surg. 2013 May;57(5):1261-8, 1268.e1-5. doi: 10.1016/j.jvs.2012.11.039. Epub 2013 Feb 4. J Vasc Surg. 2013. PMID: 23384493 Free PMC article.
-
Systematic review and meta-analysis of sex differences in outcomes after endovascular aneurysm repair for infrarenal abdominal aortic aneurysm.J Vasc Surg. 2020 Jan;71(1):283-296.e4. doi: 10.1016/j.jvs.2019.06.105. Epub 2019 Aug 26. J Vasc Surg. 2020. PMID: 31466739
References
-
- Hassan M, Tuckman HP, Patrick RH, Kountz DS, Kohn JL. Hospital length of stay and probability of acquiring infection. Int J Pharm Healthc Mark 2010;4:324–38. 10.1108/17506121011095182 - DOI
-
- van Rijn M, Buurman BM, Macneil Vroomen JL, Suijker JJ, ter Riet G, Moll van Charante EP, et al. . Changes in the in-hospital mortality and 30-day post-discharge mortality in acutely admitted older patients: retrospective observational study. Age Ageing 2016;45:41–7. 10.1093/ageing/afv165 - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
