

Determinants of long-term survival in patients with IDH-mutant gliomas
- PMID: 39316316
- PMCID: PMC11614945
- DOI: 10.1007/s11060-024-04826-9
Determinants of long-term survival in patients with IDH-mutant gliomas
Abstract
Background: Survival times of patients with IDH-mutant gliomas are variable and can extend to decades. Many studies provide progression-free rather than overall survival times and prognostic factors remain ill-defined. Here we explored characteristics of short- and long-term survivors within a cohort of patients with extended follow-up.
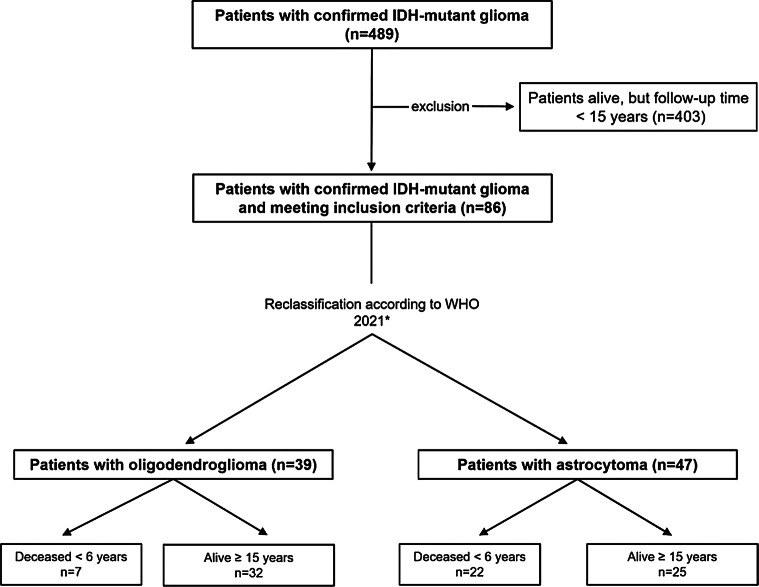
Methods: This single-center, case-control study included 86 patients diagnosed between 1998 and 2023 who either died within 6 years after diagnosis or survived at least 15 years. Patient characteristics and prognostic factors were stratified by short- (< 6 years) versus long-term (≥ 15 years) survival.
Results: Forty-seven patients (55%) diagnosed with astrocytoma and 39 patients (45%) with oligodendroglioma were included retrospectively. Median follow-up of the survivors was 16.6 years (range 15-28.9). Thirty-four deaths (40%) had been reported at database closure. Long-term survival was associated with CNS WHO grade 2 (p < 0.01), smaller tumor volumes (p = 0.01), lack of contrast enhancement (p < 0.01), wait-and-scan strategies (p < 0.01) and female sex (p = 0.04). In multivariate analyses for oligodendroglioma, larger T2 tumor volumes were associated with shorter survival (HR 1.02; 95% CI 1.01-1.05; p = 0.04). In patients with astrocytoma, lack of contrast enhancement (HR 0.38; 95% CI 0.15-0.94; p = 0.04) and wait-and-scan strategies (HR 5.75; 95% CI 1.66-26.61; p = 0.01) were associated with longer survival.
Conclusion: Large T2 tumor volume and contrast enhancement may be important risk factors for shorter survival, while age might be of lesser importance. Wait-and-scan strategies may yield excellent long-term survival in some patients with astrocytoma.
Keywords: Astrocytoma; Chemotherapy; IDH-mutation; Lower grade glioma; Oligodendroglioma; Radiotherapy; Temozolomide.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: Ethics approval was obtained by the ethics committee of the Ludwig Maximilian University of Munich (project number 20–513 and project number 21–0612). Consent to participate: Consent to participate in retrospective studies is given prospectively by all patients treated at the Department of Neurosurgery of the Ludwig Maximilian University of Munich through a local prospective tumor registry. Consent for publication: All authors have consented in submitting this manuscript for publication in the Journal of Neuro-Oncology. Additional declarations for articles in life science journals that report the results of studies involving humans and/or animals: The present study was conducted retrospectively. Competing interests: The authors declare no competing interests.
Figures
References
-
- Posti JP, Bori M, Kauko T, Sankinen M, Nordberg J, Rahi M et al (2015) Presenting symptoms of glioma in adults. Acta Neurol Scand 131(2):88–93 - PubMed
-
- Rasmussen BK, Hansen S, Laursen RJ, Kosteljanetz M, Schultz H, Norgard BM et al (2017) Epidemiology of glioma: clinical characteristics, symptoms, and predictors of glioma patients grade I-IV in the the Danish Neuro-Oncology Registry. J Neurooncol 135(3):571–579 - PubMed
-
- van den Bent MJ, Tesileanu CMS, Wick W, Sanson M, Brandes AA, Clement PM et al (2021) Adjuvant and concurrent temozolomide for 1p/19q non-co-deleted anaplastic glioma (CATNON; EORTC study 26053– 22054): second interim analysis of a randomised, open-label, phase 3 study. Lancet Oncol 22(6):813–823 - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
