

Pig-to-human kidney xenotransplants using genetically modified minipigs
- PMID: 39317190
- PMCID: PMC11513830
- DOI: 10.1016/j.xcrm.2024.101744
Pig-to-human kidney xenotransplants using genetically modified minipigs
Abstract
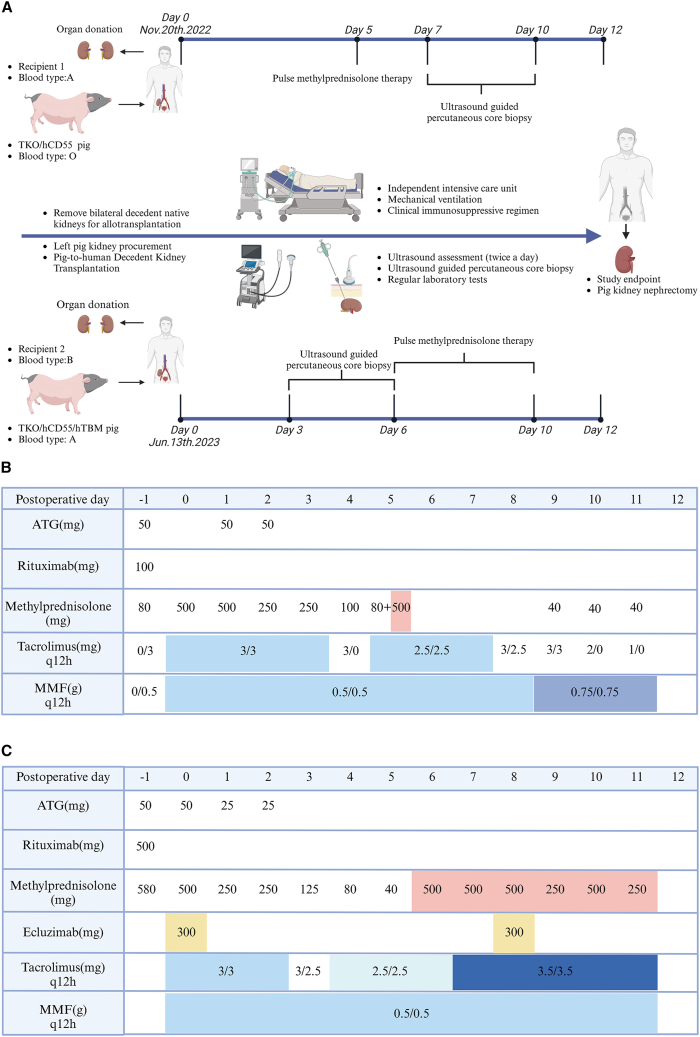
This study develops an observational model to assess kidney function recovery and xenogeneic immune responses in kidney xenotransplants, focusing on gene editing and immunosuppression. Two brain-dead patients undergo single kidney xenotransplantation, with kidneys donated by minipigs genetically modified to include triple-gene knockouts (GGTA1, β4GalNT2, CMAH) and human gene transfers (hCD55 or hCD55/hTBM). Renal xenograft functions are fully restored; however, immunosuppression without CD40-CD154 pathway blockade is ineffective in preventing acute rejection by day 12. This rejection manifests as both T cell-mediated rejection and antibody-mediated rejection (AMR), confirmed by natural killer (NK) cell and macrophage infiltration in sequential xenograft biopsies. Despite donor pigs being pathogen free before transplantation, xenografts and recipient organs test positive for porcine cytomegalovirus/porcine roseolovirus (PCMV/PRV) by the end of the observation period, indicating reactivation and contributing to significant immunopathological changes. This study underscores the critical need for extended clinical observation and comprehensive evaluation using deceased human models to advance xenograft success.
Keywords: PCMV/PRV; acute xenograft rejection; brain-dead human decedent; genetically engineered pig; kidney transplantation; xenotransplantation.
Copyright © 2024. Published by Elsevier Inc.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures






References
-
- Montgomery R.A., Stern J.M., Lonze B.E., Tatapudi V.S., Mangiola M., Wu M., Weldon E., Lawson N., Deterville C., Dieter R.A., et al. Results of two cases of pig-to-human kidney xenotransplantation. N. Engl. J. Med. 2022;386:1889–1898. - PubMed
-
- Porrett P.M., Orandi B.J., Kumar V., Houp J., Anderson D., Cozette Killian A., Hauptfeld-Dolejsek V., Martin D.E., Macedon S., Budd N., et al. First clinical-grade porcine kidney xenotransplant using a human decedent model. Am. J. Transplant. 2022;22:1037–1053. - PubMed
-
- Moazami N., Stern J.M., Khalil K., Kim J.I., Narula N., Mangiola M., Weldon E.P., Kagermazova L., James L., Lawson N., et al. Pig-to-human heart xenotransplantation in two recently deceased human recipients. Nat. Med. 2023;29:1989–1997. - PubMed
-
- Loupy A., Goutaudier V., Giarraputo A., Mezine F., Morgand E., Robin B., Khalil K., Mehta S., Keating B., Dandro A., et al. Immune response after pig-to-human kidney xenotransplantation: a multimodal phenotyping study. Lancet. 2023;402:1158–1169. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
