

Feasibility, safety and preliminary efficacy of preoperative stereotactic radiotherapy on the future pancreatic neck transection margin to reduce the risk of pancreatic fistula after high-risk pancreatoduodenectomy (FIBROPANC): protocol for a multicentre, single-arm trial
- PMID: 39317507
- PMCID: PMC11423754
- DOI: 10.1136/bmjopen-2024-087193
Feasibility, safety and preliminary efficacy of preoperative stereotactic radiotherapy on the future pancreatic neck transection margin to reduce the risk of pancreatic fistula after high-risk pancreatoduodenectomy (FIBROPANC): protocol for a multicentre, single-arm trial
Abstract
Introduction: Postoperative pancreatic fistula (POPF) occurs in 25% of patients undergoing a high-risk pancreatoduodenectomy (PD) and is a driving cause of major morbidity, mortality, prolonged hospital stay and increased costs after PD. There is a need for perioperative methods to decrease these risks. In recent studies, preoperative chemoradiotherapy in patients with pancreatic ductal adenocarcinoma (PDAC) reduced the rate of POPF seemingly due to radiation-induced pancreatic fibrosis. However, patients with a high risk of POPF mostly have a non-pancreatic periampullary tumour and do not receive radiotherapy. Prospective studies using radiotherapy specifically to reduce the risk of POPF have not been performed. We aim to assess the safety, feasibility and preliminary efficacy of preoperative stereotactic radiotherapy on the future pancreatic neck transection margin to reduce the rate of POPF.
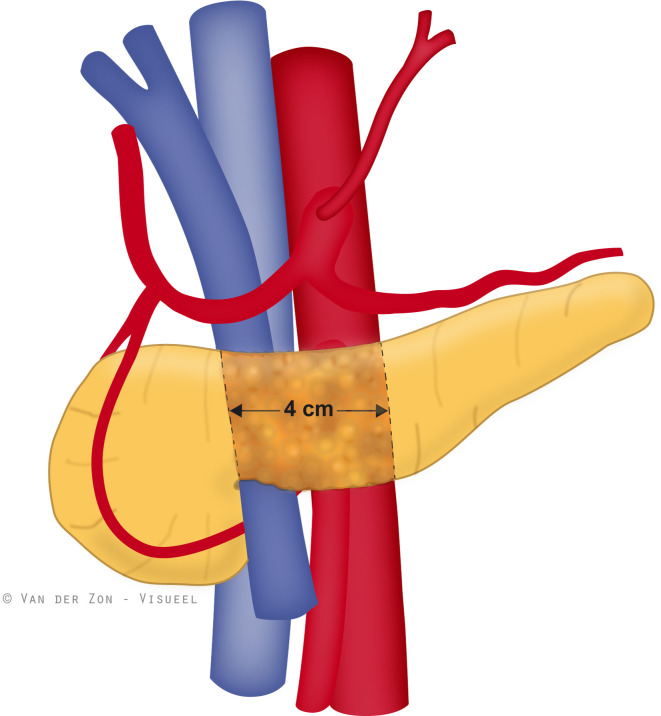
Methods and analysis: In this multicentre, single-arm, phase II trial, we aim to assess the feasibility and safety of a single fraction of preoperative stereotactic radiotherapy (12 Gy) to a 4 cm area around the future pancreatic neck transection margin in patients at high risk of developing POPF after PD aimed to reduce the risk of grade B/C POPF. Adult patients scheduled for PD for malignant and premalignant periampullary tumours, excluding PDAC, with a pancreatic duct diameter ≤3 mm will be included in centres participating in the Dutch Pancreatic Cancer Group. The primary outcome is the safety and feasibility of single-dose preoperative stereotactic radiotherapy before PD. The most relevant secondary outcomes are grade B/C POPF and the difference in the extent of fibrosis between the radiated and non-radiated (uncinate margin) pancreas. Evaluation of endpoints will be performed after inclusion of 33 eligible patients.
Ethics and dissemination: Ethical approval was obtained by the Amsterdam UMC's accredited Medical Research Ethics Committee (METC). All included patients are required to have provided written informed consent. The results of this trial will be used to determine the need for a randomised controlled phase III trial and submitted to a high-impact peer-reviewed medical journal regardless of the study outcome.
Trial registration number: NL72913 (Central Committee on Research involving Human Subjects Registry) and NCT05641233 (ClinicalTrials).
Keywords: clinical trials; hepatobiliary disease; pancreatic disease; pancreatic surgery; radiotherapy.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Smits FJ, Henry AC, Besselink MG, et al. Algorithm-based care versus usual care for the early recognition and management of complications after pancreatic resection in the Netherlands: an open-label, nationwide, stepped-wedge cluster-randomised trial. Lancet. 2022;399:1867–75. doi: 10.1016/S0140-6736(22)00182-9. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical