

Cost-effectiveness analysis of segmental adrenal venous sampling with radiofrequency ablation for primary aldosteronism in Japan
- PMID: 39317867
- PMCID: PMC11790736
- DOI: 10.1007/s11604-024-01665-6
Cost-effectiveness analysis of segmental adrenal venous sampling with radiofrequency ablation for primary aldosteronism in Japan
Abstract
Purpose: The purpose of this study was to evaluate the cost-effectiveness of comprehensive treatment strategy, including segmental adrenal venous sampling (sAVS) and radiofrequency ablation (RFA), versus medication-only strategy for primary aldosteronism.
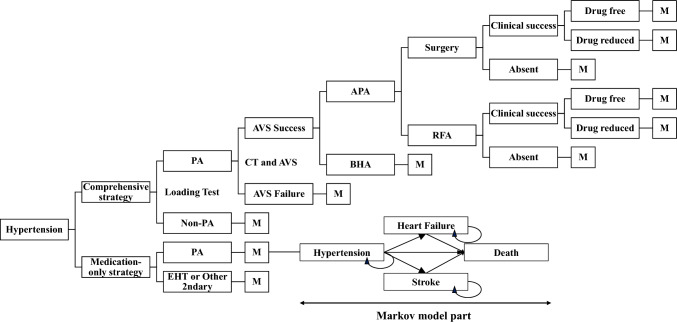
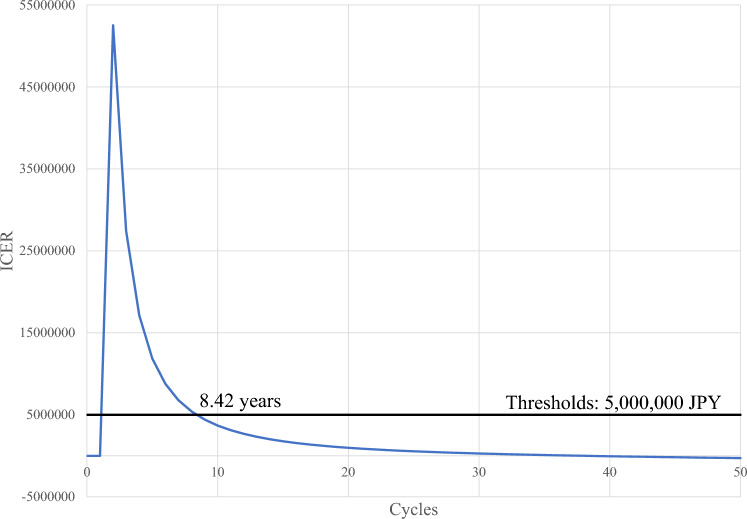
Materials and methods: A Markov decision model was developed to compare the cost-effectiveness of a comprehensive treatment strategy and a medication-only strategy for 50-year-old men and women with stage I-III hypertension. The comprehensive treatment strategy included aldosterone/renin ratio measurement, two loading tests, computed tomography, sAVS, drugs, surgery, and RFA. We built a model with a yearly cycle over 32- and 38-year time horizons for men and women, respectively, and four health states: hypertension, heart failure, stroke, and death. The incremental cost-effectiveness ratio (ICER), expressed as Japanese yen per quality-adjusted life-years (QALYs), was estimated, and strategy preference was determined on the basis of 5 million Japanese yen per QALY societal willingness-to-pay threshold.
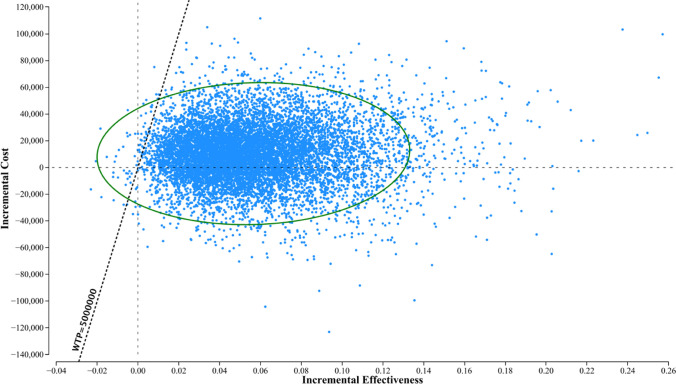
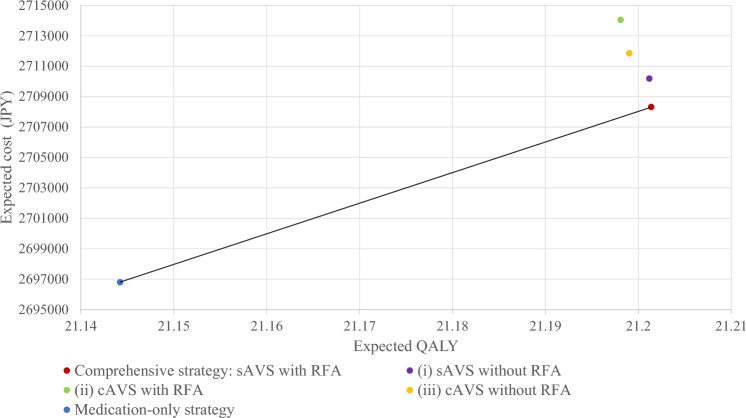
Results: The ICERs of the comprehensive treatment strategy over the medication-only strategy were 201,482 and 3,399 JPY per QALY for men and women, respectively. The resultant ICER was less than the 5 million JPY societal willingness-to-pay threshold. Deterministic sensitivity analysis and probabilistic sensitivity analysis revealed that the results varied with the input values, but the comprehensive strategy was likely to be more cost-effective than the medication-only strategy.
Conclusion: This cost-effectiveness study revealed that a comprehensive treatment strategy including sAVS and RFA was favorable compared with the medication-only strategy for managing stage I-III hypertension in 50-year-old men and women, with acceptable willingness-to-pay thresholds. This cost-effectiveness study revealed that a comprehensive treatment strategy for primary aldosteronism that included segmental adrenal sampling and radiofrequency ablation was favorable compared with the medication-only strategy for managing stage I-III hypertension in 50-year-old men and women, with acceptable willingness-to-pay thresholds.
Keywords: Adrenal venous sampling; Cost-effectiveness analysis; Primary aldosteronism; Radiofrequency ablation.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: Kei Takase and Hideki Ota were supported by a research grant from Canon Medical Systems. The other authors report no conflicts of interest.
Figures

Similar articles
-
Cost-Effectiveness Analysis of the Diagnosis and Treatment of Primary Aldosteronism in Japan.Horm Metab Res. 2015 Oct;47(11):826-32. doi: 10.1055/s-0035-1559645. Epub 2015 Aug 25. Horm Metab Res. 2015. PMID: 26305168
-
Cost-effectiveness analysis of radiofrequency renal denervation for uncontrolled hypertension in Canada.J Med Econ. 2025 Dec;28(1):70-80. doi: 10.1080/13696998.2024.2441072. Epub 2024 Dec 19. J Med Econ. 2025. PMID: 39660790
-
Cost-effectiveness analysis of radiofrequency renal denervation for uncontrolled hypertension in Sweden.Blood Press. 2025 Dec;34(1):2487583. doi: 10.1080/08037051.2025.2487583. Epub 2025 Apr 11. Blood Press. 2025. PMID: 40162937
-
Radiofrequency Ablation Technology in Liver Malignancies: A Systematic Review of Economic Evaluations.J Gastrointest Cancer. 2025 Jun 12;56(1):135. doi: 10.1007/s12029-025-01256-2. J Gastrointest Cancer. 2025. PMID: 40504321 Review.
-
Multi-gene Pharmacogenomic Testing That Includes Decision-Support Tools to Guide Medication Selection for Major Depression: A Health Technology Assessment.Ont Health Technol Assess Ser. 2021 Aug 12;21(13):1-214. eCollection 2021. Ont Health Technol Assess Ser. 2021. PMID: 34484487 Free PMC article.
References
-
- Ministry of Health, Labour and Welfare: Statistics & Other Data [Internet]. [cited 2022 Aug 31]. Available from: https://www.mhlw.go.jp/english/database/compendia.html
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903–13. - PubMed
-
- Nishikawa T, Omura M, Saito J, Matsuzawa Y. Primary aldosteronism: comparison between guidelines of the Japanese and the US Endocrine Society. Expert Rev Endocrinol Metab. 2012;7:637–45. - PubMed
-
- Miyake Y, Tanaka K, Nishikawa T, Naruse M, Takayanagi R, Sasano H, et al. Prognosis of primary aldosteronism in Japan: results from a nationwide epidemiological study. Endocr J. 2014;61:35–40. - PubMed
-
- Naruse M, Katabami T, Shibata H, Sone M, Takahashi K, Tanabe A, et al. Japan endocrine society clinical practice guideline for the diagnosis and management of primary aldosteronism 2021. Endocr J. 2022;69:327–59. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
