

Complex Interplay of COVID-19 ARDS with Guillain-Barré Syndrome and Cerebral Infarction: A Case Study
- PMID: 39318068
- PMCID: PMC11441711
- DOI: 10.12659/AJCR.944390
Complex Interplay of COVID-19 ARDS with Guillain-Barré Syndrome and Cerebral Infarction: A Case Study
Abstract
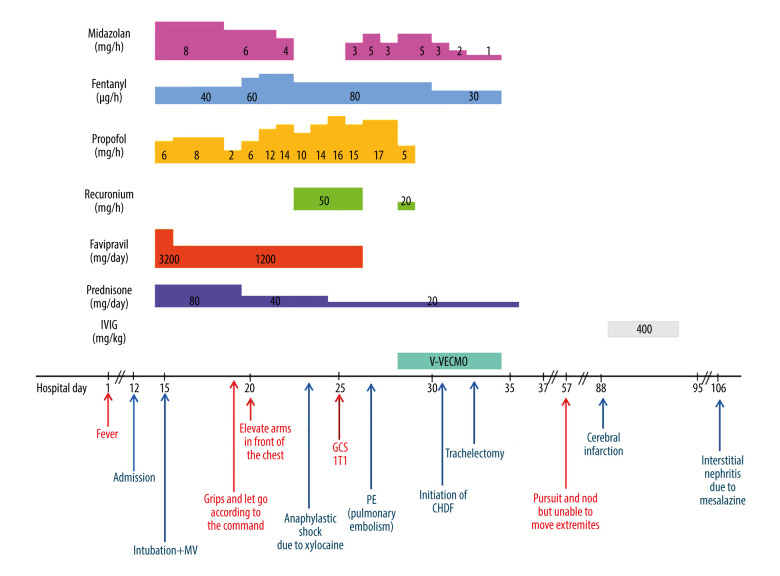
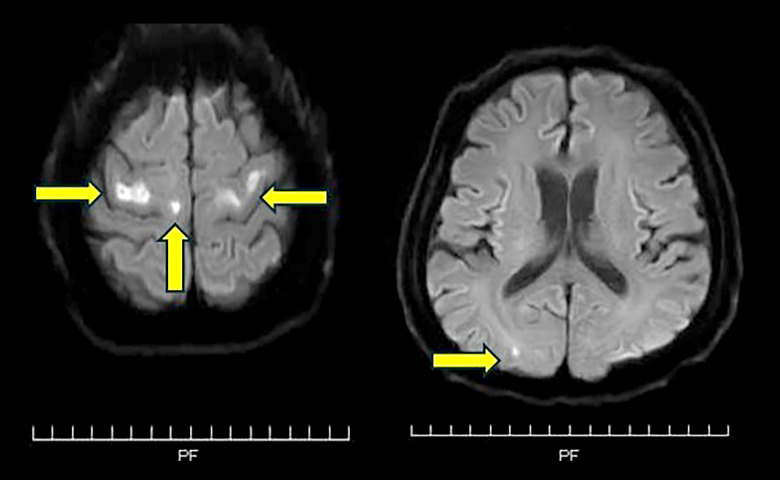
BACKGROUND Coronavirus disease (COVID-19) can cause various complications. We report a case of severe COVID-19 acute respiratory distress syndrome (ARDS) in a patient receiving veno-venous extracorporeal membrane oxygenation (V-V ECMO), complicated by Guillain-Barre syndrome (GBS) and cerebral infarction, as well as pulmonary embolism. CASE REPORT A 55-year-old Japanese man with a history of ulcerative colitis was admitted for COVID-19. His respiratory status worsened and progressed to ARDS, requiring intubation on hospital day (HD) 3. On HD 16, contrast computed tomography revealed PE. On HD 18, his respiratory condition worsened, and V-V ECMO was initiated. On HD 23, V-V ECMO was successfully discontinued. He regained consciousness on HD 44, but he had quadriplegia. Deep-tendon reflexes were absent in all limbs. Cranial nerve involvement, specifically bilateral facial nerve weakness, was noted. Magnetic resonance imaging showed bilateral scattered cerebral infarctions on HD 76. Nerve conduction studies indicated severe axonal neuropathy. Cerebrospinal fluid examination showed albuminocytologic dissociation. The antibody to the ganglioside GD1a was positive. These findings were consistent with the diagnosis of GBS. He received immunoglobulin treatment on HD 89, and his neurological findings slightly improved. CONCLUSIONS This study emphasized that in COVID-19, neurological complications are not rare, are difficult to diagnose, and are prone to delays in detection.
Conflict of interest statement
Figures
Similar articles
-
Axonal Guillain-Barre syndrome associated with SARS-CoV-2 infection in a child.J Med Virol. 2021 Sep;93(9):5599-5602. doi: 10.1002/jmv.27018. Epub 2021 Apr 23. J Med Virol. 2021. PMID: 33851741 Free PMC article.
-
Veno-venous extracorporeal membrane oxygenation for perioperative management of infective endocarditis after COVID-19 with acute respiratory distress syndrome: a case report.J Cardiothorac Surg. 2024 Jun 24;19(1):358. doi: 10.1186/s13019-024-02890-w. J Cardiothorac Surg. 2024. PMID: 38915030 Free PMC article.
-
A Case of Guillain-Barré Syndrome Associated With COVID-19.J Investig Med High Impact Case Rep. 2020 Jan-Dec;8:2324709620961198. doi: 10.1177/2324709620961198. J Investig Med High Impact Case Rep. 2020. PMID: 32981333 Free PMC article.
-
Is Guillain-Barrè syndrome triggered by SARS-CoV-2? Case report and literature review.Neurol Sci. 2021 Feb;42(2):607-612. doi: 10.1007/s10072-020-04553-9. Epub 2020 Jul 9. Neurol Sci. 2021. PMID: 32643136 Free PMC article. Review.
-
Guillain-Barré syndrome with associated unilateral ptosis without ophthalmoplegia - a rare presentation: a case report and review of the literature.J Med Case Rep. 2019 Jul 20;13(1):221. doi: 10.1186/s13256-019-2157-x. J Med Case Rep. 2019. PMID: 31324211 Free PMC article. Review.
References
-
- Gregson NA, Koblar S, Hughes RA. Antibodies to gangliosides in Guillain-Barré syndrome: Specificity and relationship to clinical features. Q J Med. 1993;86(2):111–17. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
