

Successful Treatment of Central Retinal Artery Occlusion With Tissue Plasminogen Activator Followed by Recurrent Retinal Ischemia
- PMID: 39318984
- PMCID: PMC11418660
- DOI: 10.1177/24741264241267376
Successful Treatment of Central Retinal Artery Occlusion With Tissue Plasminogen Activator Followed by Recurrent Retinal Ischemia
Abstract
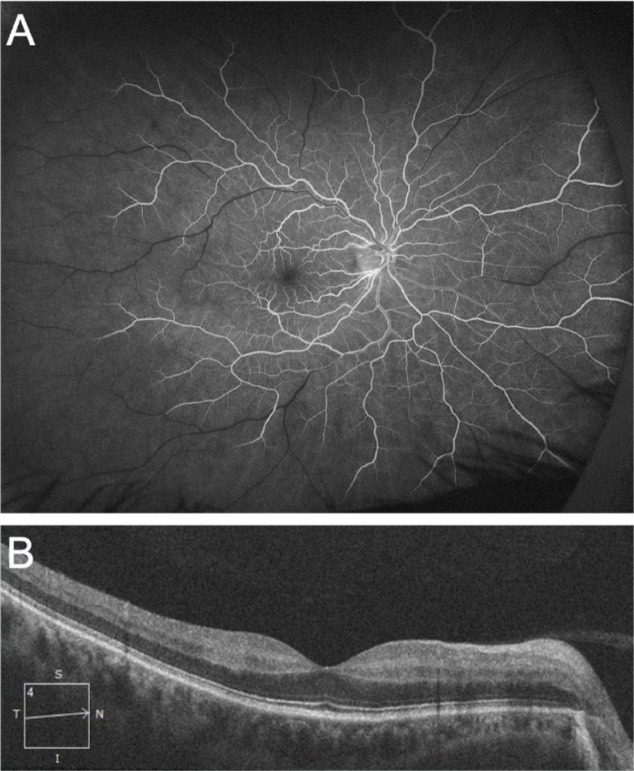
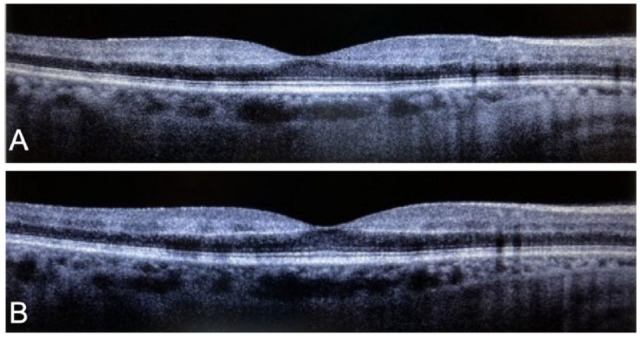
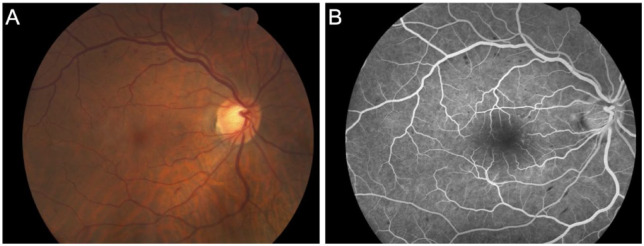
Purpose: To describe the use of intra-arterial tissue plasminogen activator (tPA) to treat central retinal artery occlusion (CRAO). Methods: A case and its findings were analyzed. Results: A 45-year-old man diagnosed with a CRAO and had cerebral angiography and treatment with intra-arterial tPA. After treatment, follow-up included optical coherence tomography (OCT), fundus photography, fluorescein angiography, and OCT angiography. The visual acuity (VA) improved from hand motions to 20/30 immediately after fibrinolysis. A vascular occlusion event the next day resulted in a decrease in VA to 20/400. After initiation of dual antiplatelet therapy, the patient's VA improved to 20/20. As the retina recovered, the evolution of retinal ischemic changes to a finding similar to paracentral acute middle maculopathy was seen on imaging. Conclusions: This is the first report describing a patient safely started on dual antiplatelet therapy that led to vision improvement after initial treatment with intra-arterial tPA for a CRAO resulted in recurrent vision loss.
Keywords: central retinal artery occlusion (CRAO); eye stroke; fibrinolysis; paracentral acute middle maculopathy (PAMM); tissue plasminogen activator (tPA).
© The Author(s) 2024.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Figures


Similar articles
-
Case Report: Paracentral acute middle maculopathy following carotid artery dissection.Front Cardiovasc Med. 2025 Jun 6;12:1560482. doi: 10.3389/fcvm.2025.1560482. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40547505 Free PMC article.
-
Prognostic factors for acute central retinal artery occlusion treated with hyperbaric oxygen: The Hong Kong study report number five.World J Methodol. 2025 Jun 20;15(2):96777. doi: 10.5662/wjm.v15.i2.96777. eCollection 2025 Jun 20. World J Methodol. 2025. PMID: 40548218 Free PMC article.
-
Optical coherence tomography (OCT) for detection of macular oedema in patients with diabetic retinopathy.Cochrane Database Syst Rev. 2015 Jan 7;1(1):CD008081. doi: 10.1002/14651858.CD008081.pub3. Cochrane Database Syst Rev. 2015. PMID: 25564068 Free PMC article.
-
Successful intra-arterial thrombolysis for central retinal artery occlusion secondary to chronic internal carotid artery occlusion: a case report.BMC Ophthalmol. 2025 Jul 10;25(1):404. doi: 10.1186/s12886-025-04248-9. BMC Ophthalmol. 2025. PMID: 40640788 Free PMC article.
-
Optical coherence tomography (OCT) for detection of macular oedema in patients with diabetic retinopathy.Cochrane Database Syst Rev. 2011 Jul 6;(7):CD008081. doi: 10.1002/14651858.CD008081.pub2. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2015 Jan 07;1:CD008081. doi: 10.1002/14651858.CD008081.pub3. PMID: 21735421 Updated.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
