

AERIFY-1/2: two phase 3, randomised, controlled trials of itepekimab in former smokers with moderate-to-severe COPD
- PMID: 39319046
- PMCID: PMC11417606
- DOI: 10.1183/23120541.00718-2023
AERIFY-1/2: two phase 3, randomised, controlled trials of itepekimab in former smokers with moderate-to-severe COPD
Abstract
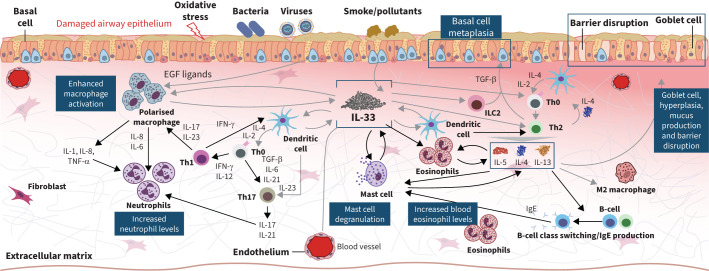
Background: Accumulating data implicate interleukin (IL)-33, a proinflammatory cytokine released locally upon epithelial cell damage, in the pathogenesis of COPD. In a phase 2 study, itepekimab, a human monoclonal antibody against IL-33, reduced exacerbations and improved lung function in a subgroup analysis of former smokers with COPD with an acceptable safety profile.
Methods: The study designs of AERIFY-1 and AERIFY-2 are described in this article.
Discussion: The primary objective of AERIFY-1/2 (NCT04701983/NCT04751487), two phase 3 randomised, double-blind, placebo-controlled trials, is to assess the efficacy and safety of itepekimab versus placebo in a population of former smokers with moderate-to-severe COPD over up to 52 weeks. An additional secondary population of current smokers are being enrolled in AERIFY-2. These two studies will enrol patients (aged 40-85 years) with COPD and chronic bronchitis who had ≥2 moderate or ≥ 1 severe exacerbations within the previous year despite standard-of-care triple or double background therapy. All participants are required to have ≥10-pack-year smoking history, and ≥6 months since smoking cessation for former smokers. The primary end-point is the annualised rate of moderate or severe acute exacerbation of COPD. Secondary end-points include change from baseline in pre- and post-bronchodilator forced expiratory volume in 1 s, and annualised frequency of severe exacerbations. Symptomatic end-points include Evaluating Respiratory Symptoms in COPD and St. George's Respiratory Questionnaire, safety and anti-drug antibody responses.
Copyright ©The authors 2024.
Conflict of interest statement
Conflict of interest: K.F. Rabe reports consultancy, speaker fees’ and advisory board membership for AstraZeneca, Boehringer Ingelheim, Chiesi, Gilead, GSK, Novartis, Pearl, Sanof and Teva; and is cofounder of rnatics, Germany. Conflict of interest: F.J. Martinez has been on steering committees for Afferent/Merck, AstraZeneca, Bayer, Boehringer Ingelheim, Gilead, GlaxoSmithKline, Nitto Pharma, Patara Pharma/Respivant Sciences, Pearl Pharmaceuticals, ProMedior/Roche, ProMetic Life Sciences, Stromedix/Biogen and Veracyte; has been an advisory board member for AstraZeneca, BioScale/ProTerrix Bio, Boehringer Ingelheim, Chiesi, CSL Behring, Gala Therapeutics, Genentech, GlaxoSmithKline, Novartis, Pearl Pharmaceuticals, Physicians Education Resource, Sunovion, Teva and Zambon; has been a consultant for Bridge Biotherapeutics, Bristol Myers Squibb and twoXR; reports continuing medical education presentation support from the Canadian Respiratory Network, Chiesi, CME Outfitters, Dartmouth University, France Foundation, Inova Fairfax, MD Magazine, Methodist Hospital, Miller Communications, National Association for Continuing Education/Haymarket, New York University, PeerView, Prime Education, Rare Diseases Healthcare Communication, Rockpointe, University of Alabama at Birmingham, UpToDate, Vindico Pharmaceuticals, WebMD/MedScape and Zambon; and has been on the data and safety monitoring board for Boehringer Ingelheim and GlaxoSmithKline. Conflict of interest: S.P. Bhatt has served on advisory boards for Boehringer Ingelheim and Regeneron, received consulting fees from Sanofi, and reports fees for continuing medical education from IntegrityCE. Conflict of interest: T. Kawayama reports support from GSK, AstraZeneca, Novartis Pharma and Healios. Conflict of interest: B.G. Cosio has served as a consultant and received speaker fees from AstraZeneca, Boehringer Ingelheim, Novartis, Chiesi, Menarini, GSK, Sanofi and Teva. Conflict of interest: R.M. Mroz reports support from AstraZeneca, Boehringer Ingelheim, Chiesi, Genentech, MSD, Gilead, GSK, Novartis, Pearl Pharmaceuticals, Sanofi and Teva. Conflict of interest: M.M. Boomsma, H. Goulaouic, M. Djandji, Y. Liu, C.R. Xu and H. Staudinger are Sanofi employees and may hold stock and/or stock options in the company. Conflict of interest: M.C. Nivens, X. Soler, M.P. Kosloski and D.J. Lederer are Regeneron Pharmaceuticals Inc. employees and shareholders. Conflict of interest: N. Amin is a prior employee and shareholder for Regeneron Pharmaceuticals Inc. Conflict of interest: R.M. Abdulai is a prior employee and stock holder for Sanofi.
Figures


References
-
- Global Initiative for Chronic Obstructive Lung Diseases (GOLD). G lobal Strategy for Diagnosis, Management and Prevention of COPD 2023 Report . Date last updated: 17 February 2023. Date last accessed: 3 April 2023. https://goldcopd.org/wp-content/uploads/2024/02/GOLD-2024_v1.2-11Jan24_W...
LinkOut - more resources
Full Text Sources