

Ureteral endometriosis: MR imaging appearance for predicting complex procedures
- PMID: 39319158
- PMCID: PMC11419901
- DOI: 10.1016/j.heliyon.2024.e34884
Ureteral endometriosis: MR imaging appearance for predicting complex procedures
Abstract
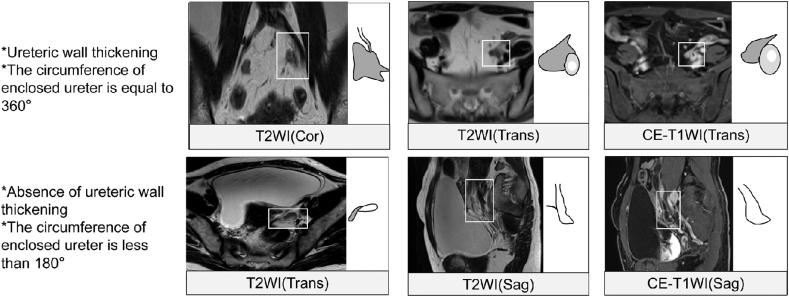
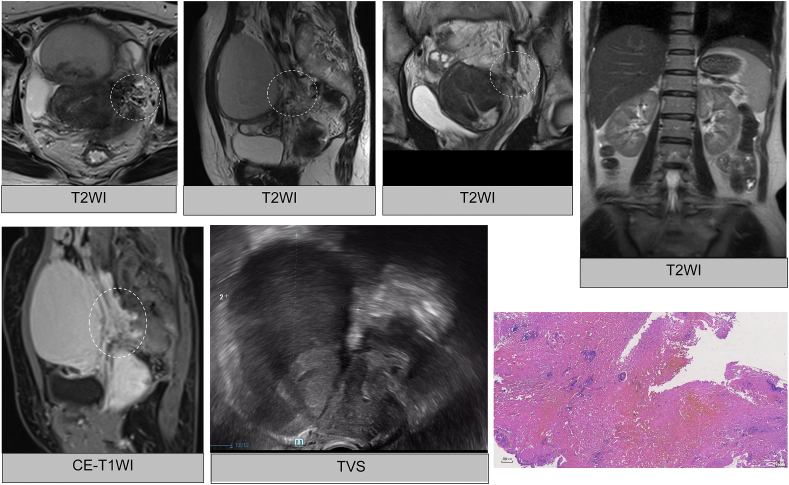
Rationale and objectives: To describe MRI characteristics of ureteral endometriosis (UE) in identifying intrinsic involvement of the ureteric wall and predicting complex procedures.
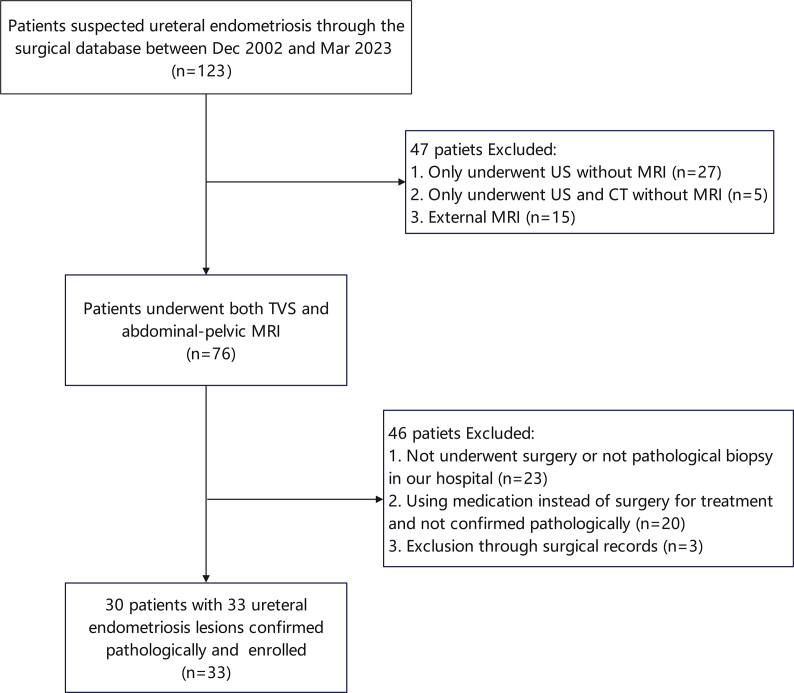
Methods: Thirty-three UE lesions in 30 patients treated for UE over a 20-year period were reviewed. A systematic analysis of 13 MRI (ureteric wall thickening, circumference, T1 signal, T2 signal, ureterectasis, lateral parametrial endometriosis (LPE), rectal endometriosis, the foregoing three-characteristic diameter, ovarian endometriomas, adenomyosis, paraurethral endometriosis) and 5 clinical (age, BMI, CA125, creatinine and rAFS stage) characteristics was performed. MRI results were compared to histology and surgical procedure performed (simple versus complex ureteral procedures).
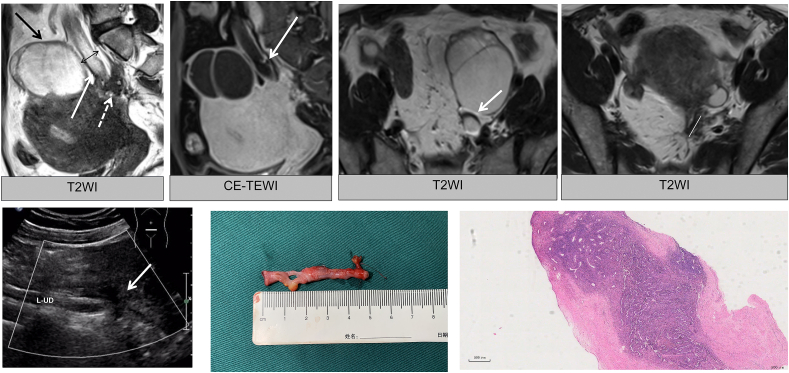
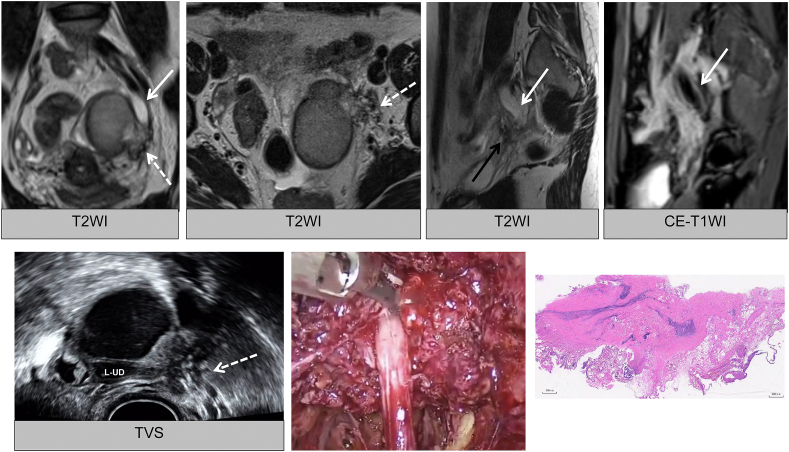
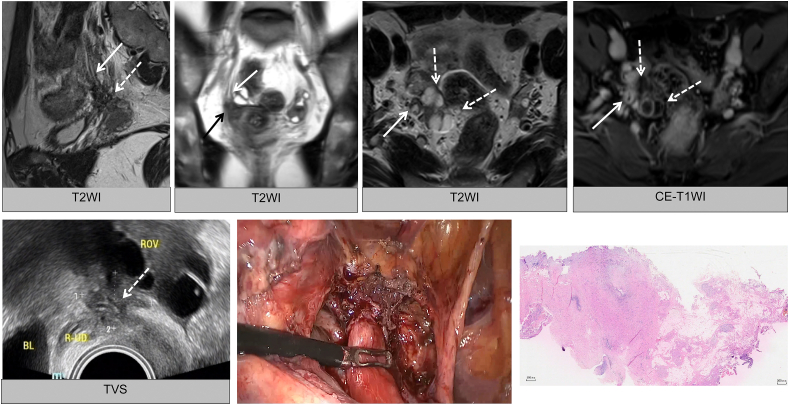
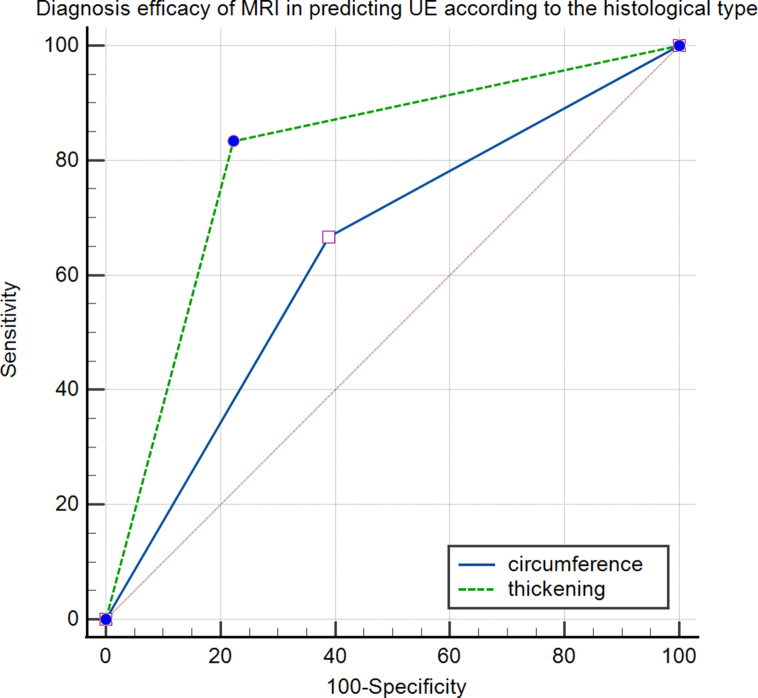
Results: Twenty-five extrinsic and 8 intrinsic UE were pathologically identified. Twenty lesions underwent a simple procedure, and 12 underwent a complex procedure, with 1 ureteroscopic biopsy. There were significant differences in the characteristics of ureteric wall thickening, the diameter of dilated ureter and LPE, rectal endometriosis and adenomyosis between extrinsic and intrinsic UE (p < 0.05). UE was associated with LPE (p = 0.033). The criteria of ureteral wall thickening more accurately predicted intrinsic UE than circumference, but the AUC was not significant difference (AUC, 0.806 and 0.639; 95 % CI, [0.594, 0.937] and [0.419, 0.823], respectively; p = 0.350). There were significant differences in creatinine, thickening and adenomyosis between the simple and complex procedures (p < 0.05). In 11 lesions with the absence of ureterectasis, 4 lesions with hydronephrosis and thickening were intrinsic and underwent complex procedures, while 7 lesions extrinsic and simple.
Conclusions: Ureteric wall thickening as a analytical criterion may accurately predict intrinsic UE and complex ureteric procedures.
Keywords: Endometriosis; Magnetic resonance imaging; Surgical procedure; Ureter.
© 2024 Published by Elsevier Ltd.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Different patterns of pelvic ureteral endometriosis. What is the best treatment? Results of a retrospective analysis.Arch Ital Urol Androl. 2016 Dec 30;88(4):266-269. doi: 10.4081/aiua.2016.4.266. Arch Ital Urol Androl. 2016. PMID: 28073190
-
Histological evaluation of ureteral involvement in women with deep infiltrating endometriosis: analysis of a large series.Hum Reprod. 2015 Apr;30(4):833-9. doi: 10.1093/humrep/deu360. Epub 2015 Jan 12. Hum Reprod. 2015. PMID: 25586785
-
[Ureteric and bladder involvement of deep pelvic endometriosis. Value of multidisciplinary surgical management].Prog Urol. 2006 Nov;16(5):588-93. Prog Urol. 2006. PMID: 17175957 French.
-
Laparoscopic Treatment of Ureteral Endometriosis: A Systematic Review.J Minim Invasive Gynecol. 2021 Apr;28(4):779-787. doi: 10.1016/j.jmig.2020.11.022. Epub 2020 Nov 27. J Minim Invasive Gynecol. 2021. PMID: 33253957
-
Ureteral endometriosis: a systematic review of epidemiology, pathogenesis, diagnosis, treatment, risk of malignant transformation and fertility.Hum Reprod Update. 2018 Nov 1;24(6):710-730. doi: 10.1093/humupd/dmy027. Hum Reprod Update. 2018. PMID: 30165449
Cited by
-
Optimizing endometriosis detection: a review of technical approaches and interpretative pitfalls.Abdom Radiol (NY). 2025 Jun 27. doi: 10.1007/s00261-025-05084-7. Online ahead of print. Abdom Radiol (NY). 2025. PMID: 40576666 Review.
References
-
- Vercellini P., Vigano P., Somigliana E., et al. Endometriosis: pathogenesis and treatment. Nat. Rev. Endocrinol. 2014;10:261–275. - PubMed
-
- Clement P.B. The pathology of endometriosis: a survey of the many faces of a common disease emphasizing diagnostic pitfalls and unusual and newly appreciated aspects. Adv. Anat. Pathol. 2007;14:241–260. - PubMed
-
- Bazot M., Daraï E. Diagnosis of deep endometriosis: clinical examination, ultrasonography, magnetic resonance imaging, and other techniques. Fertil. Steril. 2017;108:886–894. - PubMed
-
- Shenoy-Bhangle A.S., Pires-Franco I.V., Ray L.J., et al. Imaging of urinary bladder and ureteral endometriosis with emphasis on diagnosis and technique. Acad. Radiol. 2023;23:6. 00608. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
