

Prediction of Severe Baseline Asymptomatic Carotid Stenosis and Subsequent Risk of Stroke and Cardiovascular Disease
- PMID: 39319460
- PMCID: PMC11518973
- DOI: 10.1161/STROKEAHA.123.046894
Prediction of Severe Baseline Asymptomatic Carotid Stenosis and Subsequent Risk of Stroke and Cardiovascular Disease
Abstract
Background: Risk models to identify patients at high risk of asymptomatic carotid artery stenosis (ACAS) can help in selecting patients for screening, but long-term outcomes in these patients are unknown. We assessed the diagnostic and prognostic value of the previously published Prevalence of ACAS (PACAS) risk model to detect ACAS at baseline and to predict subsequent risk of stroke and cardiovascular disease (CVD) during follow-up.
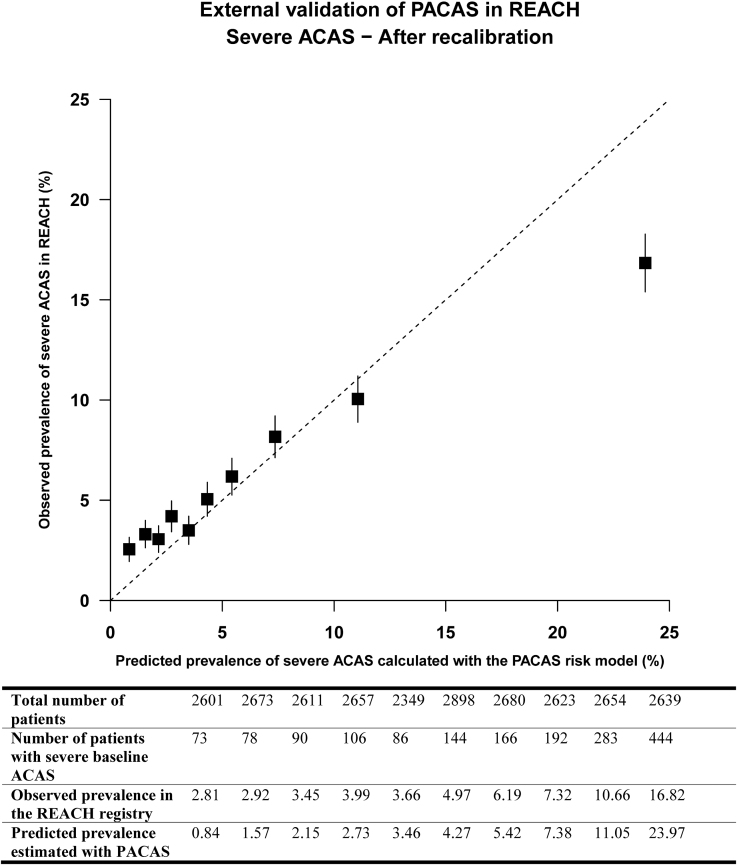
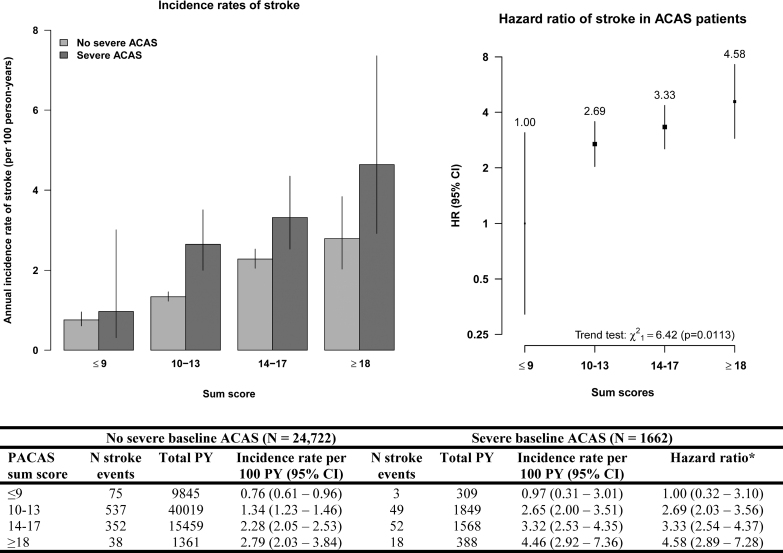
Methods: We validated the discrimination and calibration of the PACAS risk model to detect severe (≥70% narrowing) ACAS with patients from the Reduction of Atherothrombosis for Continued Health registry. We subsequently calculated the incidence rates of stroke and CVD (fatal and nonfatal stroke or myocardial infarction or vascular death) during follow-up in 4 risk groups (low, medium, high, and very high, corresponding to sum scores of ≤9, 10-13, 14-17, and ≥18, respectively).
Results: Among 26 384 patients, aged between 45 and 80 years, without prior carotid procedures, 1662 (6.3%) had severe baseline ACAS. During ≈70 000 patient-years of follow-up, 1124 strokes and 2484 CVD events occurred. Discrimination of the PACAS model was 0.67 (95% CI, 0.65-0.68), and calibration showed adequate concordance between predicted and observed risks of severe baseline ACAS after recalibration. Significantly higher incidence rates of stroke (Ptrend<0.011) and CVD (Ptrend<0.0001) during follow-up were found with increasing PACAS risk groups. Among patients with high PACAS sum score of ≥14 (corresponding to 27.7% of all patients), severe baseline ACAS prevalence was 11.4%. In addition, 56.6% of incident strokes and 64.9% of incident CVD events occurred in this group.
Conclusions: The PACAS risk model can reliably identify patients at high risk of severe baseline ACAS. Incidence rates of stroke and CVD during follow-up were significantly higher in patients with high PACAS sum scores. Selective screening of patients with high PACAS sum scores may help to prevent future stroke or CVD.
Keywords: asymptomatic diseases; cardiovascular diseases; carotid stenosis; epidemiologic methods; mass screening; risk assessment; stroke.
Conflict of interest statement
Dr Bhatt discloses the following relationships: advisory board: Angiowave, Bayer, Boehringer Ingelheim, CellProthera, Cereno Scientific, Elsevier Practice Update Cardiology, High Enroll, Janssen, Level Ex, McKinsey, Medscape Cardiology, Merck, MyoKardia, NirvaMed, Novo Nordisk, PhaseBio, PLx Pharma, and Stasys; board of directors: American Heart Association New York City, Angiowave (stock options), Bristol Myers Squibb (stock), DRS.LINQ (stock options), and High Enroll (stock); consultant: Broadview Ventures, Hims, SFJ, and Youngene; data monitoring committees: Acesion Pharma, Assistance Publique-Hôpitaux de Paris, Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute, for the PORTICO trial [Portopulmonary Hypertension Treatment With Macitentan: A Randomized Clinical Trial], funded by St. Jude Medical, now Abbott), Boston Scientific (chair: the PEITHO trial [Pulmonary Embolism Thrombolysis]), Cleveland Clinic, Contego Medical (chair: PERFORMANCE 2 [Protection Against Emboli During Carotid Artery Stenting Using the Neuroguard IEP System]), Duke Clinical Research Institute, Mayo Clinic, Mount Sinai School of Medicine (for the ENVISAGE trial, funded by Daiichi Sankyo; for the ABILITY-DM trial, funded by Concept Medical; for ALLAY-HF [Safety and Efficacy of the Alleviant System for No-Implant Interatrial Shunt Creation in Patients With Chronic Heart Failure], funded by Alleviant Medical), Novartis, Population Health Research Institute, and Rutgers University (for the National Institutes of Health-funded MINT trial [Myocardial Ischemia and Transfusion]); honoraria: American College of Cardiology (senior associate editor: Clinical Trials and News, ACC.org; chair: ACC Accreditation Oversight Committee), Arnold and Porter law firm (work related to Sanofi/Bristol Myers Squibb clopidogrel litigation), Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute; the RE-DUAL PCI [Evaluation of Dual Therapy With Dabigatran vs Triple Therapy With Warfarin in Patients With AF That Undergo a PCI With Stenting] Clinical Trial Steering Committee funded by Boehringer Ingelheim; AEGIS-II [Study to Investigate CSL112 in Subjects With Acute Coronary Syndrome] Executive Committee funded by CSL Behring), Belvoir Publications (editor-in-chief: Harvard Heart Letter), Canadian Medical and Surgical Knowledge Translation Research Group (clinical trial steering committees), CSL Behring (AHA lecture), Cowen and Company, Duke Clinical Research Institute (clinical trial steering committees, including for the PRONOUNCE trial [A Trial Comparing Cardiovascular Safety of Degarelix Versus Leuprolide in Patients With Advanced Prostate Cancer and Cardiovascular Disease], funded by Ferring Pharmaceuticals), HMP Global (editor-in-chief:
Figures

Comment in
-
Risk Models for the Detection of Severe Asymptomatic Carotid Stenosis and the Prediction of Future Strokes and Cardiovascular Events.Stroke. 2024 Nov;55(11):2641-2642. doi: 10.1161/STROKEAHA.124.048875. Epub 2024 Sep 25. Stroke. 2024. PMID: 39319452 No abstract available.
References
-
- Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Bäck M, Benetos A, Biffi A, Boavida JM, Capodanno D, et al. ; ESC National Cardiac Societies. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021;42:3227–3337. doi: 10.1093/eurheartj/ehab484 - PubMed
-
- Hadar N, Raman G, Moorthy D, O’Donnell TF, Thaler DE, Feldmann E, Lau J, Kitsios GD, Dahabreh IJ. Asymptomatic carotid artery stenosis treated with medical therapy alone: temporal trends and implications for risk assessment and the design of future studies. Cerebrovasc Dis. 2014;38:163–173. doi: 10.1159/000365206 - PubMed
-
- Poorthuis MHF, Solomon Y, Herings RAR, Visseren FLJ, Kappelle LJ, Bots ML, Rissanen I, de Borst GJ. Temporal trends and determinants of stroke risk in patients with medically treated asymptomatic carotid stenosis. Stroke. 2023;54:1735–1749. doi: 10.1161/STROKEAHA.122.041921 - PubMed
-
- Naylor R, Rantner B, Ancetti S, de Borst GJ, De Carlo M, Halliday A, Kakkos SK, Markus HS, McCabe DJH, Sillesen H, et al. . Editor’s choice - European Society for Vascular Surgery (ESVS) 2023 clinical practice guidelines on the management of atherosclerotic carotid and vertebral artery disease. Eur J Vasc Endovasc Surg. 2023;65:7–111. doi: 10.1016/j.ejvs.2022.04.011 - PubMed
-
- AbuRahma AF, Avgerinos ED, Chang RW, Darling RC, 3rd, Duncan AA, Forbes TL, Malas MB, Murad MH, Perler BA, Powell RJ, et al. . Society for vascular surgery clinical practice guidelines for management of extracranial cerebrovascular disease. J Vasc Surg. 2022;75:4s–22s. doi: 10.1016/j.jvs.2021.04.073 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
