

MEDI1814 selectively reduces free Aβ42 in cerebrospinal fluid of non-clinical species and Alzheimer's disease patients
- PMID: 39319998
- PMCID: PMC11567870
- DOI: 10.1002/alz.14238
MEDI1814 selectively reduces free Aβ42 in cerebrospinal fluid of non-clinical species and Alzheimer's disease patients
Abstract
Introduction: Small molecules and antibodies are being developed to lower amyloid beta (Aβ) peptides.
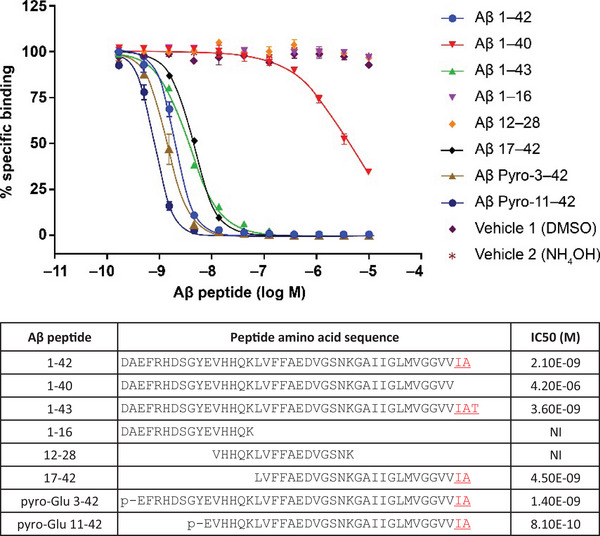
Methods: We describe MEDI1814, a fully human high-affinity monoclonal antibody selective for Aβ42, the pathogenic self-aggregating species of Aβ.
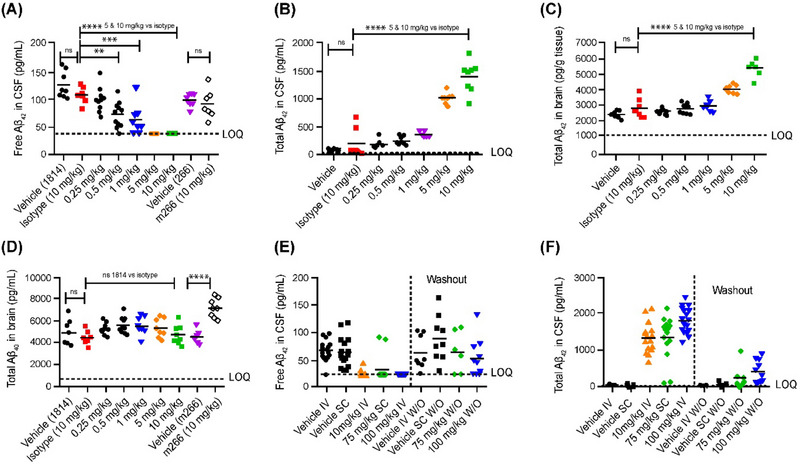
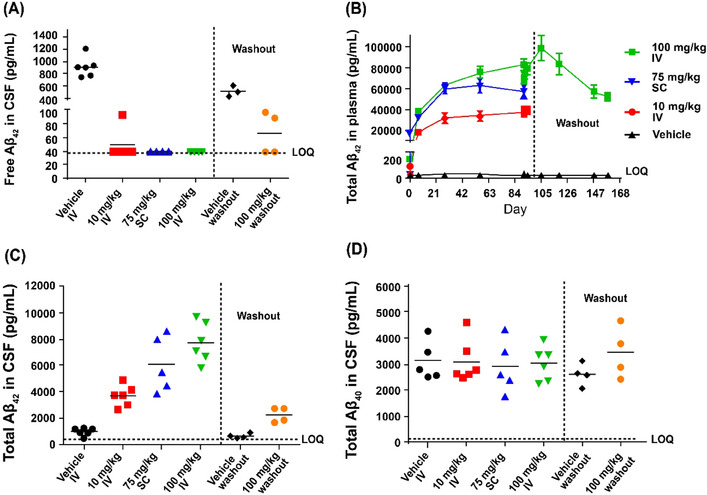
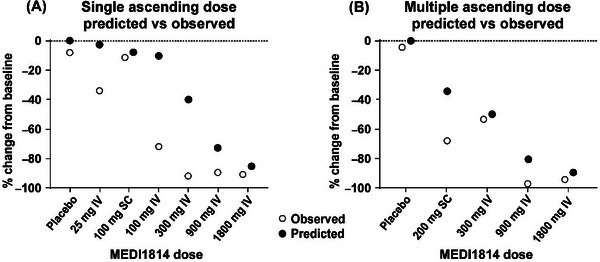
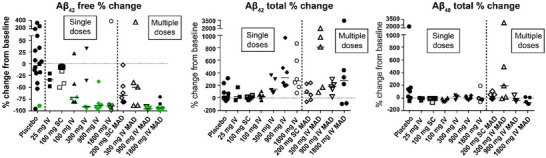
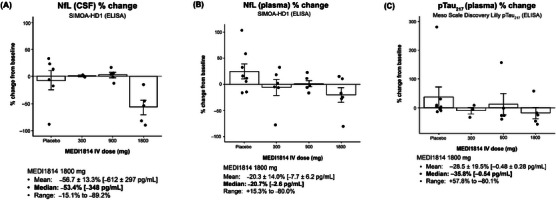
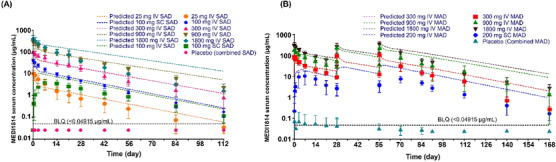
Results: MEDI1814 reduces free Aβ42 without impacting Aβ40 in the cerebrospinal fluid of rats and cynomolgus monkeys after systemic administration. MEDI1814 administration to patients with Alzheimer's disease (AD; n = 57) in single or repeat doses up to 1800 mg intravenously or 200 mg subcutaneously was associated with a favorable safety and tolerability profile. No cases of amyloid-related imaging abnormalities were observed. Predictable dose-proportional changes in serum exposures for MEDI1814 were observed across cohorts. Cerebrospinal fluid (CSF) analysis demonstrated central nervous system penetration of MEDI1814. Pharmacodynamic data showed dose-dependent suppression of free Aβ42, increases in total (bound and free) Aβ42, but no change in total Aβ40 in CSF across doses.
Discussion: MEDI1814 offers a differentiated approach to impacting Aβ in AD via selective reduction of free Aβ42.
Keywords: amyloid beta 42; drug development; pharmacodynamics; pharmacokinetics; preclinical; safety; tolerability.
© 2024 The Author(s). Alzheimer's & Dementia published by Wiley Periodicals LLC on behalf of Alzheimer's Association.
Conflict of interest statement
CL, PN, DL, AN, ABo, SE, SG, FW, TC, MMcF, RVB, RT, MSP, ZSV, EL, MP, ADD, TJV, MTG, CS, KT, TO, IPC, and ABi are either current or former employees of AstraZeneca, and either own or owned shares/options in AstraZeneca. P‐OF is an inventor on patents or patent applications. FN, YF, JRS, NKP, and JLD are current or former employees of Eli Lilly. JLD is an inventor on patents or patent applications of Eli Lilly and Company relating to the assays, methods, reagents and / or compositions of matter for p‐tau assays. JLD has served as a consultant or on advisory boards for Eisai, Abbvie, Genotix Biotechnologies Inc, Gates Ventures, Karuna Therapeutics, AlzPath Inc., Cognito Therapeutics, Inc., and received research support from ADx Neurosciences, Fujirebio, AlzPath Inc., Roche Diagnostics, and Eli Lilly and Company in the past 2 years. JLD has received speaker fees from Eli Lilly and Company. JLD is a founder and advisor for Monument Biosciences. JLD has stock or stock options in Eli Lilly and Company, Genotix Biotechnologies, AlzPath Inc., and Monument Biosciences. MEDI1814 is covered by PCT patent application WO2014060444. KH has nothing to declare. Author disclosures are available in the supporting information.
Figures
References
-
- World Health Organization . Dementia. 2022.
-
- Braak H, Del Tredici K. The pathological process underlying Alzheimer's disease in individuals under thirty. Acta Neuropathol. 2011;121:171‐181. - PubMed
-
- Hardy JA, Higgins GA. Alzheimer's disease: the amyloid cascade hypothesis. Science. 1992;256:184‐185. - PubMed
-
- Hardy J. Testing times for the “amyloid cascade hypothesis”. Neurobiol Aging. 2002;23:1073‐1074. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
