

Prediction of High Nodal Burden in Patients With Sentinel Node-Positive Luminal ERBB2-Negative Breast Cancer
- PMID: 39320882
- PMCID: PMC11425194
- DOI: 10.1001/jamasurg.2024.3944
Prediction of High Nodal Burden in Patients With Sentinel Node-Positive Luminal ERBB2-Negative Breast Cancer
Abstract
Importance: In patients with clinically node-negative (cN0) breast cancer and 1 or 2 sentinel lymph node (SLN) macrometastases, omitting completion axillary lymph node dissection (CALND) is standard. High nodal burden (≥4 axillary nodal metastases) is an indication for intensified treatment in luminal breast cancer; hence, abstaining from CALND may result in undertreatment.
Objective: To develop a prediction model for high nodal burden in luminal ERBB2-negative breast cancer (all histologic types and lobular breast cancer separately) without CALND.
Design, setting, and participants: The prospective Sentinel Node Biopsy in Breast Cancer: Omission of Axillary Clearance After Macrometastases (SENOMAC) trial randomized patients 1:1 to CALND or its omission from January 2015 to December 2021 among adult patients with cN0 T1-T3 breast cancer and 1 or 2 SLN macrometastases across 5 European countries. The cohort was randomly split into training (80%) and test (20%) sets, with equal proportions of high nodal burden. Prediction models were developed by multivariable logistic regression in the complete luminal ERBB2-negative cohort and a lobular breast cancer subgroup. Nomograms were constructed. The present diagnostic/prognostic study presents the results of a prespecified secondary analysis of the SENOMAC trial. Herein, only patients with luminal ERBB2-negative tumors assigned to CALND were selected. Data analysis for this article took place from June 2023 to April 2024.
Exposure: Predictors of high nodal burden.
Main outcomes and measures: High nodal burden was defined as ≥4 axillary nodal metastases. The luminal prediction model was evaluated regarding discrimination and calibration.
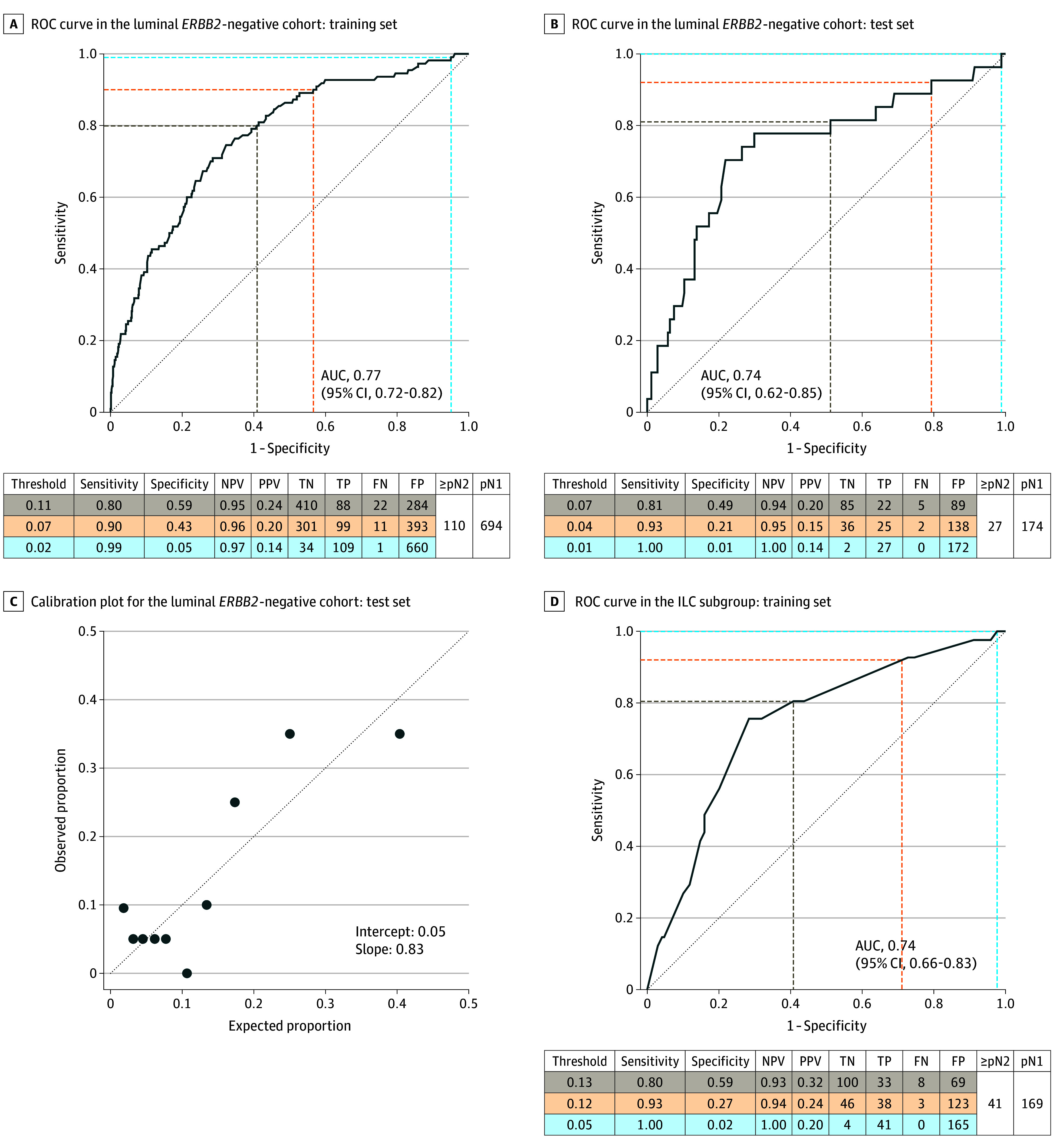
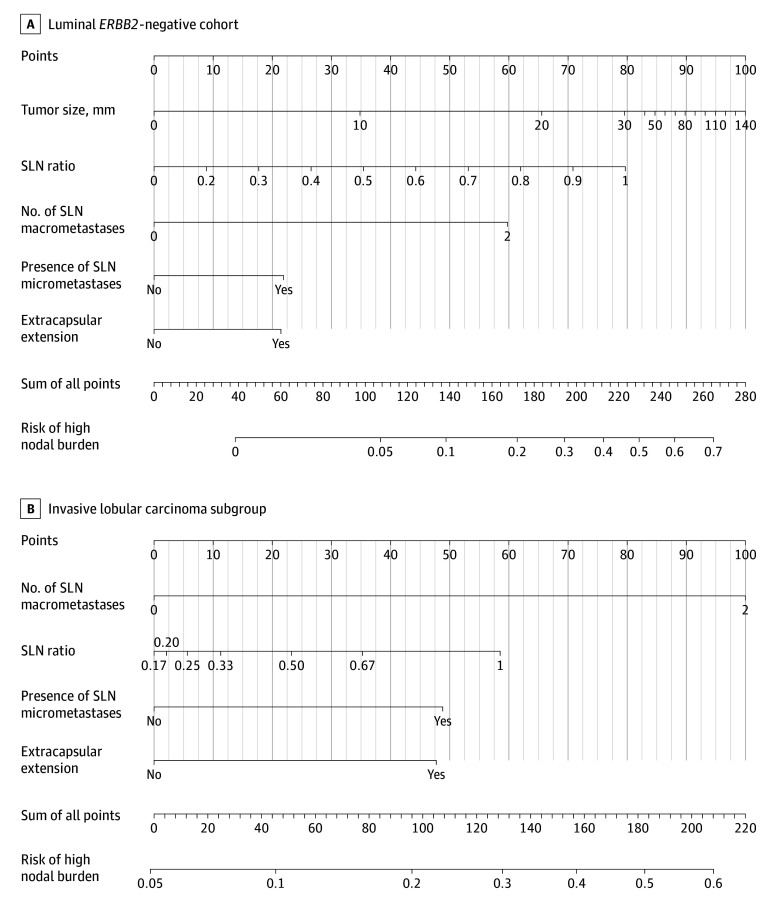
Results: Of 1010 patients (median [range] age, 61 [34-90] years; 1006 [99.6%] female and 4 [0.4%] male), 138 (13.7%) had a high nodal burden and 212 (21.0%) had lobular breast cancer. The model in the training set (n = 804) included number of SLN macrometastases, presence of SLN micrometastases, SLN ratio, presence of SLN extracapsular extension, and tumor size (not included in lobular subgroup). Upon validation in the test set (n = 201), the area under the receiver operating characteristic curve (AUC) was 0.74 (95% CI, 0.62-0.85) and the calibration was satisfactory. At a sensitivity threshold of ≥80%, all but 5 low-risk patients were correctly classified corresponding to a negative predictive value of 94%. The prediction model for the lobular subgroup reached an AUC of 0.74 (95% CI, 0.66-0.83).
Conclusions and relevance: The predictive models and nomograms may facilitate systemic treatment decisions without exposing patients to the risk of arm morbidity due to CALND. External validation is needed.
Trial registration: ClinicalTrials.gov Identifier: NCT02240472.
Conflict of interest statement
Figures
Comment on
-
Importance of Cooperation Between Cooperative Group Clinical Trialists.JAMA Surg. 2024 Dec 1;159(12):1403. doi: 10.1001/jamasurg.2024.3926. JAMA Surg. 2024. PMID: 39320930 No abstract available.
References
-
- Giuliano AE, Ballman KV, McCall L, et al. . Effect of axillary dissection vs no axillary dissection on 10-year overall survival among women with invasive breast cancer and sentinel node metastasis: the ACOSOG Z0011 (Alliance) randomized clinical trial. JAMA. 2017;318(10):918-926. doi:10.1001/jama.2017.11470 - DOI - PMC - PubMed
-
- Galimberti V, Cole BF, Zurrida S, et al. ; International Breast Cancer Study Group Trial 23-01 investigators . Axillary dissection versus no axillary dissection in patients with sentinel-node micrometastases (IBCSG 23-01): a phase 3 randomised controlled trial. Lancet Oncol. 2013;14(4):297-305. doi:10.1016/S1470-2045(13)70035-4 - DOI - PMC - PubMed
-
- Donker M, van Tienhoven G, Straver ME, et al. . Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer (EORTC 10981-22023 AMAROS): a randomised, multicentre, open-label, phase 3 non-inferiority trial. Lancet Oncol. 2014;15(12):1303-1310. doi:10.1016/S1470-2045(14)70460-7 - DOI - PMC - PubMed
-
- Burstein HJ, Curigliano G, Loibl S, et al. ; Members of the St. Gallen International Consensus Panel on the Primary Therapy of Early Breast Cancer 2019 . Estimating the benefits of therapy for early-stage breast cancer: the St. Gallen International Consensus Guidelines for the primary therapy of early breast cancer 2019. Ann Oncol. 2019;30(10):1541-1557. doi:10.1093/annonc/mdz235 - DOI - PubMed
-
- Johnston SRD, Harbeck N, Hegg R, et al. ; MONARCHE Committee Members and Investigators . Abemaciclib combined with endocrine therapy for the adjuvant treatment of HR+, HER2-, node-positive, high-risk, early breast cancer (MONARCHE). J Clin Oncol. 2020;38(34):3987-3998. doi:10.1200/JCO.20.02514 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
