

Clinician Willingness to Prescribe Medications for Opioid Use Disorder to Adolescents in Indiana
- PMID: 39320891
- PMCID: PMC11425143
- DOI: 10.1001/jamanetworkopen.2024.35416
Clinician Willingness to Prescribe Medications for Opioid Use Disorder to Adolescents in Indiana
Abstract
Importance: Prescribing medications for opioid use disorders (MOUD), including buprenorphine, naltrexone, and methadone, to adolescents remains an underused evidence-based strategy for reducing harms associated with opioid use.
Objective: To identify potential associations between clinician- and community-level characteristics regarding clinicians' self-reported willingness to prescribe MOUD to adolescents.
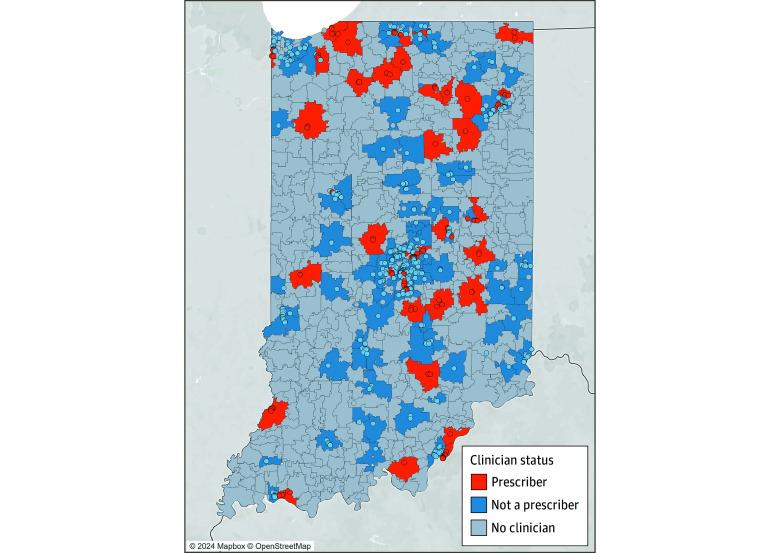
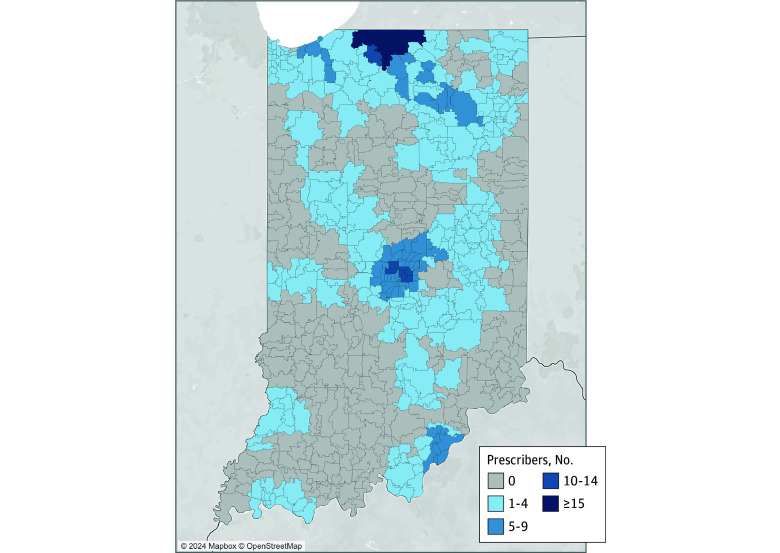
Design, setting, and participants: This cross-sectional study included a phone survey of Indiana clinicians and spatial analysis of community-level characteristics. Clinicians were eligible for inclusion in analyses if actively providing health care and listed on the Buprenorphine Practitioner Locator website, a publicly available national registry of clinicians possessing a waiver to legally prescribe buprenorphine (ie, waivered clinicians).
Exposures: Community-level characteristics, including total population, rurality or urbanicity, percentage with incomes below the federal poverty line, and racial or ethnic makeup.
Main outcomes and measures: Clinicians were asked about their willingness to prescribe MOUD to adolescents younger than 18 years if clinically indicated. Responses were recorded as no, yes, or yes with conditions.
Results: Among the 871 clinicians listed on the website as of July 2022, 832 were eligible for inclusion and contacted by phone. Among waivered clinicians, 759 (91.2%) reported being unwilling to prescribe MOUD to adolescents, 73 clinicians (8.8%) reported willingness to prescribe MOUD to adolescents, and only 24 (2.9%) would do so without conditions. A multivariable logistic regression model including spatially lagged community-level variables showed that, among areas with waivered clinicians, clinicians practicing in more populated areas were significantly less likely to prescribe to adolescents (β = 0.65; 95% CI, 0.49-0.87; P = .003). Similarly, those in more rural areas were significantly more likely to prescribe to adolescents (β = 1.27; 95% CI, 1.02-1.58; P = .03). Variation in clinician willingness to prescribe was not explained by other community-level characteristics. Among all waivered clinicians, advanced practice clinicians were less likely than physicians to report willingness to prescribe (β = 0.58; 95% CI, 0.35-0.97; P = .04), as were physicians without any specialty training relevant to MOUD prescribing when compared with family medicine clinicians (β = 0.40; 95% CI, 0.18-0.89; P = .03). A small subgroup of waivered clinicians had training in pediatrics (13 clinicians [1.6%]), and none were willing to prescribe MOUD to adolescents.
Conclusions and relevance: From this cross-sectional study, it appears that Indiana adolescents continued to face gaps in access to MOUD treatment, despite its well-established efficacy. Programs that support primary care practitioners, including family medicine clinicians and pediatricians, in safe and appropriate use of MOUD in adolescents may bridge these gaps.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
