

Predicting Response to Neuromodulators or Prokinetics in Patients With Suspected Gastroparesis Using Machine Learning: The "BMI, Infectious Prodrome, Delayed GES, and No Diabetes" Model
- PMID: 39320959
- PMCID: PMC11421729
- DOI: 10.14309/ctg.0000000000000743
Predicting Response to Neuromodulators or Prokinetics in Patients With Suspected Gastroparesis Using Machine Learning: The "BMI, Infectious Prodrome, Delayed GES, and No Diabetes" Model
Abstract
Introduction: Pharmacologic therapies for symptoms of gastroparesis (GP) have limited efficacy, and it is difficult to predict which patients will respond. In this study, we implemented a machine learning model to predict the response to prokinetics and/or neuromodulators in patients with GP-like symptoms.
Methods: Subjects with suspected GP underwent simultaneous gastric emptying scintigraphy (GES) and wireless motility capsule and were followed for 6 months. Subjects were included if they were started on neuromodulators and/or prokinetics. Subjects were considered responders if their GP Cardinal Symptom Index at 6 months decreased by ≥1 from baseline. A machine learning model was trained using lasso regression, ridge regression, or random forest. Five-fold cross-validation was used to train the models, and the area under the receiver operator characteristic curve (AUC-ROC) was calculated using the test set.
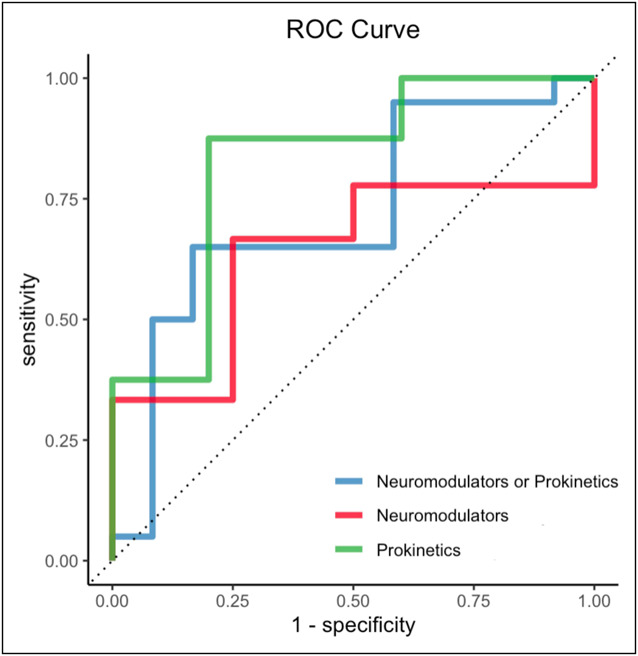
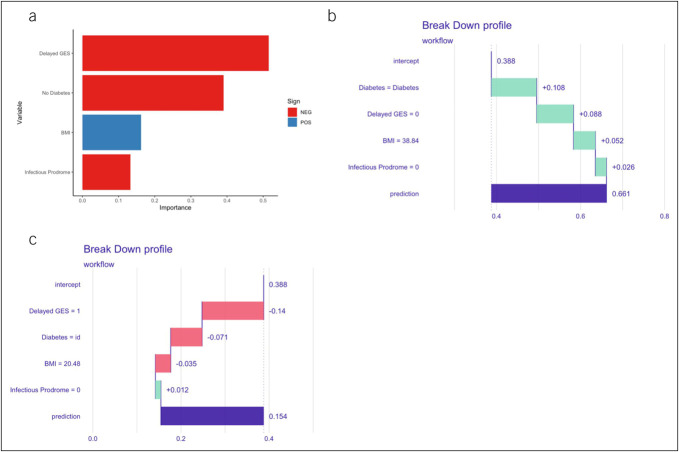
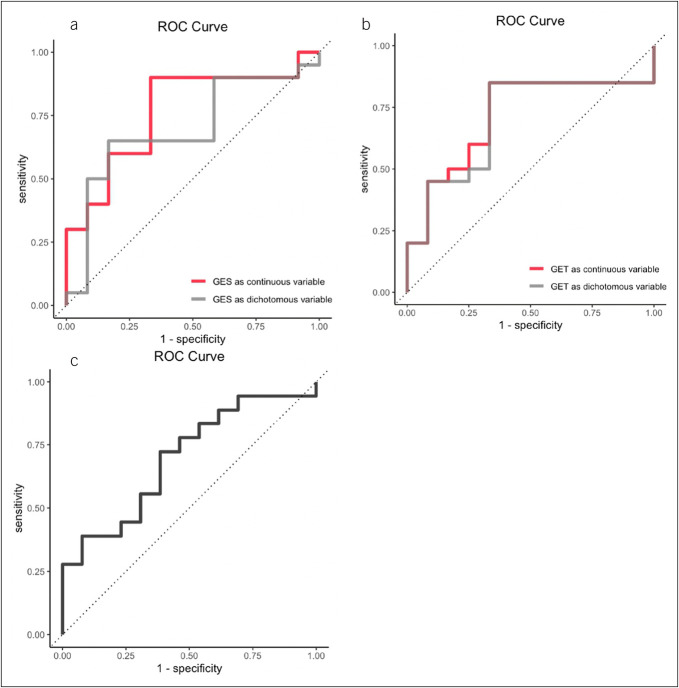
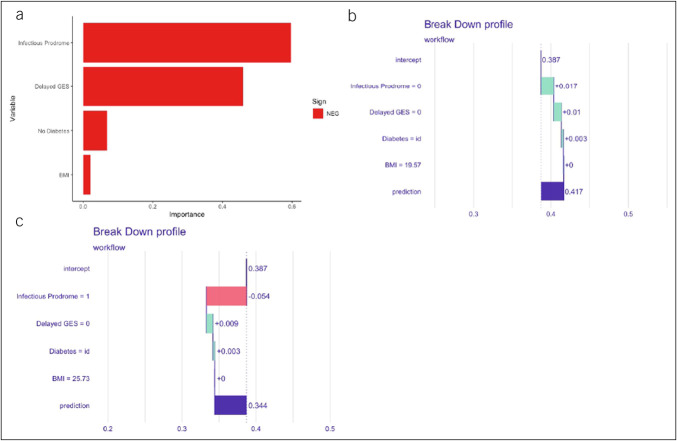
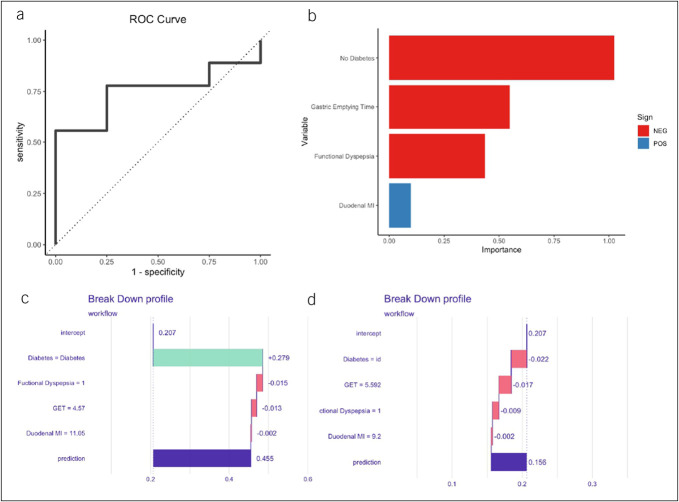
Results: Of the 150 patients enrolled, 123 patients received either a prokinetic and/or a neuromodulator. Of the 123, 45 were considered responders and 78 were nonresponders. A ridge regression model with the variables, such as body mass index, infectious prodrome, delayed gastric emptying scintigraphy, no diabetes, had the highest AUC-ROC of 0.72. The model performed well for subjects on prokinetics without neuromodulators (AUC-ROC of 0.83) but poorly for those on neuromodulators without prokinetics. A separate model with gastric emptying time, duodenal motility index, no diabetes, and functional dyspepsia performed better (AUC-ROC of 0.75).
Discussion: This machine learning model has an acceptable accuracy in predicting those who will respond to neuromodulators and/or prokinetics. If validated, our model provides valuable data in predicting treatment outcomes in patients with GP-like symptoms.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The American College of Gastroenterology.
Conflict of interest statement
Figures
References
-
- Lacy BE, Tack J, Gyawali CP. AGA clinical practice update on management of medically refractory gastroparesis: Expert review. Clin Gastroenterol Hepatol 2022;20(3):491–500. - PubMed
-
- Ingrosso MR, Camilleri M, Tack J, et al. Efficacy and safety of drugs for gastroparesis: Systematic review and network meta-analysis. Gastroenterology 2023;164(4):642–54. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
