

Multidimensional Immunotyping of Human NF1-Associated Peripheral Nerve Sheath Tumors Uncovers Tumor-Associated Macrophages as Key Drivers of Immune Evasion in the Tumor Microenvironment
- PMID: 39321200
- PMCID: PMC11866061
- DOI: 10.1158/1078-0432.CCR-24-1454
Multidimensional Immunotyping of Human NF1-Associated Peripheral Nerve Sheath Tumors Uncovers Tumor-Associated Macrophages as Key Drivers of Immune Evasion in the Tumor Microenvironment
Abstract
Purpose: Malignant peripheral nerve sheath tumors (MPNST) are aggressive soft-tissue sarcomas and the leading cause of mortality in individuals with neurofibromatosis type 1 (NF1). Despite many clinical trials, outcomes for patients with MPNST have remained stagnant, and most succumb to their disease; thus, novel therapeutic approaches are needed. A better understanding of the MPNST immune ecosystem will aid in the development of strategies to activate the immune system against the tumor. In this study, we profile the tumor immune microenvironment (TIME) in NF1-associated peripheral nerve sheath tumors (PNST) to discover insights on the role played by tumor-infiltrating immune cells in malignant transformation.
Experimental design: Using fresh and formalin-fixed paraffin-embedded tissue from patients diagnosed with NF1-PNST, we dissected the TIME through IHC, multiparameter flow cytometry, and comparative transcriptomic studies.
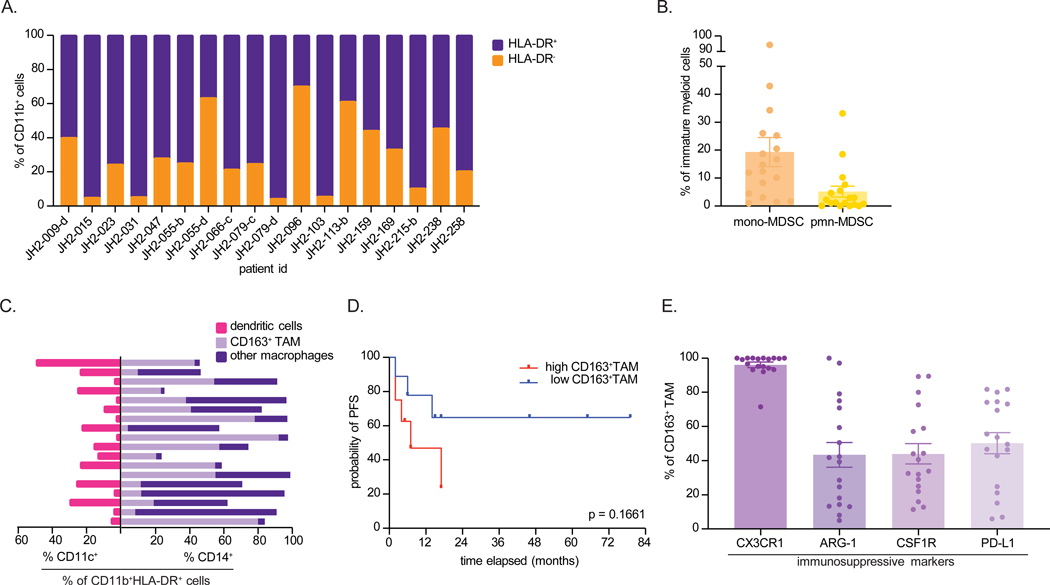
Results: Immunophenotyping confirmed increased immune cell infiltration during malignant progression, with a predominance of infiltrating myeloid cells, particularly CD163+ tumor-associated macrophages (TAM). The T cells within MPNST exhibited signs of tumor activation, characterized by high programmed cell death 1 expression. Additionally, MPNST specimens demonstrated elevated levels of immunosuppressive TAM, with heightened PD-L1 expression. The proportion of CD163+ myeloid cells within the TIME correlated with poorer progression-free survival. Notably, loss of H3K27 trimethylation correlated with low immune cell infiltration in MPNST.
Conclusions: Malignant transformation of NF1-PNST is characterized by an immunosuppressive microenvironment comprising TAM with high expression of PD-L1, which is associated with inferior outcomes. These findings suggest the clinical potential of immune-modulating therapeutics that can unleash an antitumor immune response.
©2024 American Association for Cancer Research.
Conflict of interest statement
Figures




References
-
- Hirbe AC, Gutmann DH. Neurofibromatosis type 1: a multidisciplinary approach to care. Lancet Neurol. 2014;13(8):834–43. - PubMed
-
- Miettinen MM, Antonescu CR, Fletcher CDM, Kim A, Lazar AJ, Quezado MM, et al. Histopathologic evaluation of atypical neurofibromatous tumors and their transformation into malignant peripheral nerve sheath tumor in patients with neurofibromatosis 1-a consensus overview. Hum Pathol. 2017;67:1–10. - PMC - PubMed
-
- Carli M, Ferrari A, Mattke A, Zanetti I, Casanova M, Bisogno G, et al. Pediatric malignant peripheral nerve sheath tumor: the Italian and German soft tissue sarcoma cooperative group. J Clin Oncol. 2005;23(33):8422–30. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
