

Model of integrated mental health video consultations for people with depression or anxiety in primary care (PROVIDE-C): assessor masked, multicentre, randomised controlled trial
- PMID: 39322237
- PMCID: PMC11423708
- DOI: 10.1136/bmj-2024-079921
Model of integrated mental health video consultations for people with depression or anxiety in primary care (PROVIDE-C): assessor masked, multicentre, randomised controlled trial
Abstract
Objective: To evaluate whether an integrated mental health video consultation approach (PROVIDE model) can improve symptoms compared with usual care in adults with depression and anxiety disorders attending primary care.
Design: Assessor masked, multicentre, randomised controlled trial (PROVIDE-C).
Setting: In 29 primary care practices in Germany, working remotely online from one trial hub.
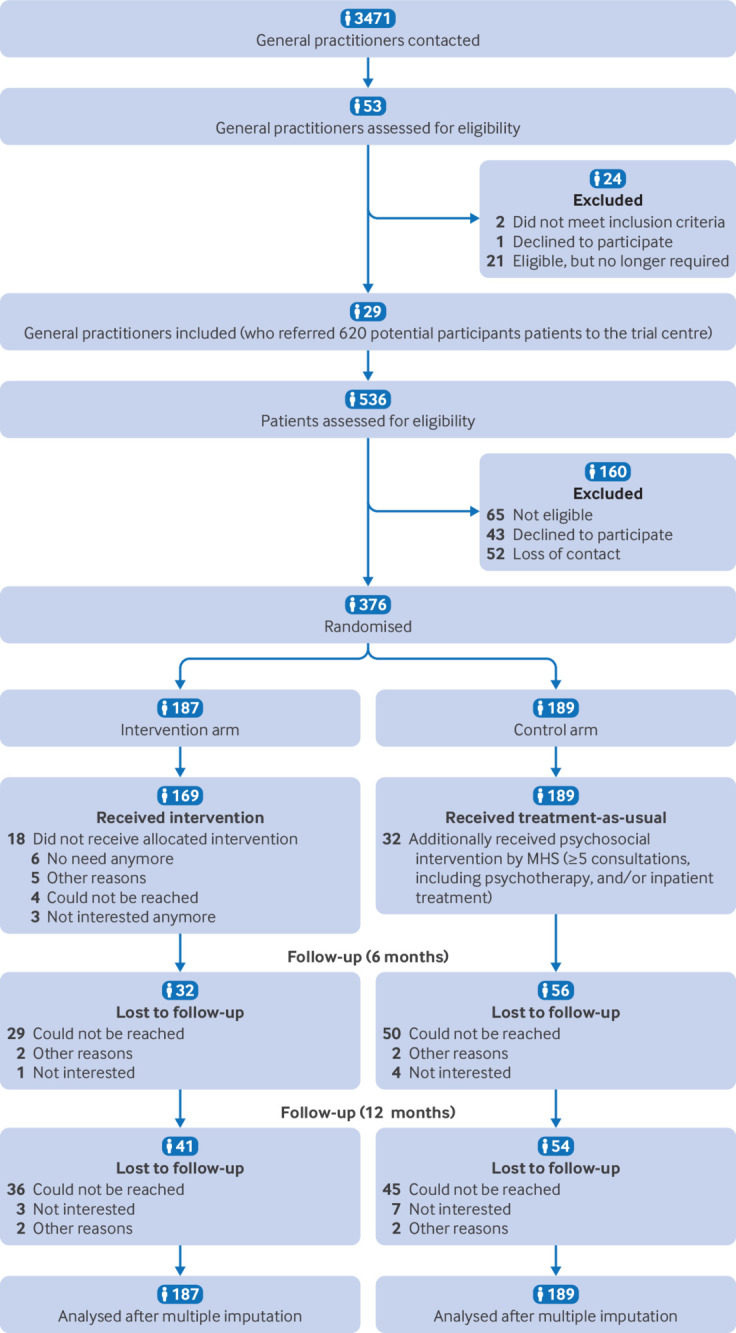
Participants: 376 adults (18-81 years) who presented to their general practitioner (GP) with depression or anxiety, or both.
Intervention: Participants were randomised (1:1) to receive the PROVIDE model (n=187) or usual care (n=189). Usual care was provided by GPs through interventions such as brief counselling and psychotropic medication prescriptions and may or may not have included referrals to mental health specialists. The PROVIDE model comprised transdiagnostic treatment provided through five real-time video sessions between the patient at the primary care practice and a mental health specialist at an offsite location.
Main outcome measures: The primary outcome was the absolute change in the mean severity of depressive and anxiety symptoms measured using the patient health questionnaire anxiety and depression scale (PHQ-ADS) at six months, in the intention-to-treat population. Secondary outcomes, measured at six and 12 months, included PHQ-ADS subscores, psychological distress related to somatic symptoms, recovery, health related quality of life, quality and patient centredness of chronic illness care, and adverse events.
Results: Between 24 March 2020 and 23 November 2021, 376 patients were randomised into treatment groups. Mean age was 45 years (standard deviation (SD) 14), 63% of the participants were female, and mean PHQ-ADS-score was 26 points (SD 7.6). Compared with usual care, the PROVIDE intervention led to improvements in severity of depressive and anxiety symptom (adjusted mean change difference in the PHQ-ADS score -2.4 points (95% confidence interval -4.5 to -0.4), P=0.02) at six months. The effects were sustained at 12 months (-2.9 (-5.0 to -0.7), P<0.01). No serious adverse events were reported in either group.
Conclusions: Through relatively low intensity treatment, the PROVIDE model led to a decrease in depressive and anxiety symptoms with small effects in the short and long term. Depression and anxiety disorders are prevalent and therefore the small effect might cumulatively impact on population health in this population.
Trial registration: ClinicalTrials.gov NCT04316572.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/and declare: funding from German Federal Ministry of Education and Research (BMBF) (grant no. 01GY16129); no financial relationships with any funding from organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have affected the submitted work.
Figures
References
-
- James SL, Abate D, Abate KH, et al. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators . Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018;392:1789-858. 10.1016/S0140-6736(18)32279-7 - DOI - PMC - PubMed
-
- World Health Organization. World mental health report: transforming mental health for all. Geneva, Switzerland: World Health Organization; 2022 June . https://archive.hshsl.umaryland.edu/handle/10713/20295