

Effect of mesenchymal stem cells on the host response in severe community-acquired pneumonia
- PMID: 39322407
- PMCID: PMC11503173
- DOI: 10.1136/thorax-2024-222026
Effect of mesenchymal stem cells on the host response in severe community-acquired pneumonia
Abstract
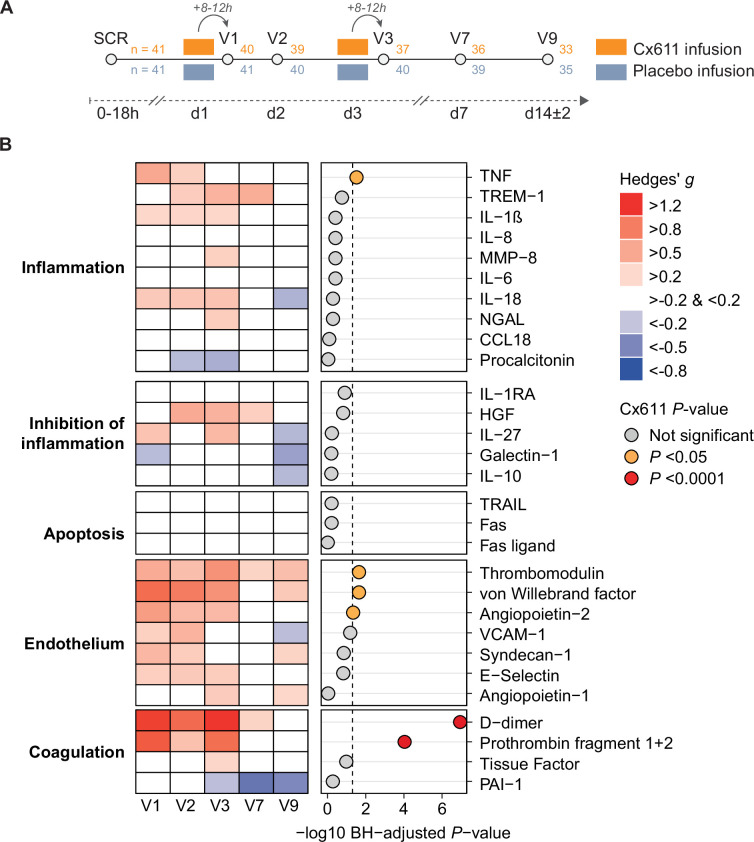
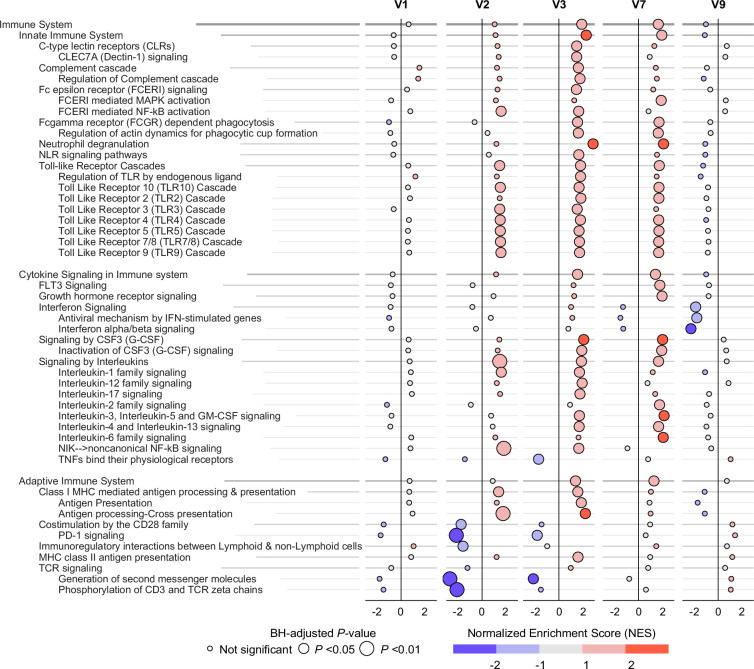
Mesenchymal stem cells (MSC) have immune regulatory properties that may ameliorate pathophysiological processes in sepsis. We determined the effect of allogeneic adipose-derived MSCs (Cx611) on the host response during sepsis due to community-acquired bacterial pneumonia (CABP) by measuring 29 plasma biomarkers and blood transcriptomes at six time points in 82 patients randomised to two intravenous infusions of Cx611 or placebo. Cx611 treatment enhanced several endothelial cell and procoagulant response plasma biomarkers, and led to increased expression of pathways related to innate immunity, haemostasis and apoptosis. Cx611 infusion in sepsis due to CABP is associated with broad host response alterations.
Keywords: Critical Care; Pneumonia.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: DVO, KJG and EL are employed by Takeda Pharmaceuticals, which produces Cx611.
Figures
References
-
- Sun J, Ding X, Sun T. Mesenchymal Stem Cells in Sepsis: From Basic Research to Clinical Application. ICRES. 2021;1:2. doi: 10.2991/icres.k.210622.001. - DOI
-
- Laterre P-F, Sánchez-García M, van der Poll T, et al. A phase Ib/IIa, randomised, double-blind, multicentre trial to assess the safety and efficacy of expanded Cx611 allogeneic adipose-derived stem cells (eASCs) for the treatment of patients with community-acquired bacterial pneumonia admitted to the intensive care unit. BMC Pulm Med. 2020;20:309. doi: 10.1186/s12890-020-01324-2. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials