

LocoMMotion: a study of real-life current standards of care in triple-class exposed patients with relapsed/refractory multiple myeloma - 2-year follow-up (final analysis)
- PMID: 39322709
- PMCID: PMC11588650
- DOI: 10.1038/s41375-024-02404-6
LocoMMotion: a study of real-life current standards of care in triple-class exposed patients with relapsed/refractory multiple myeloma - 2-year follow-up (final analysis)
Abstract
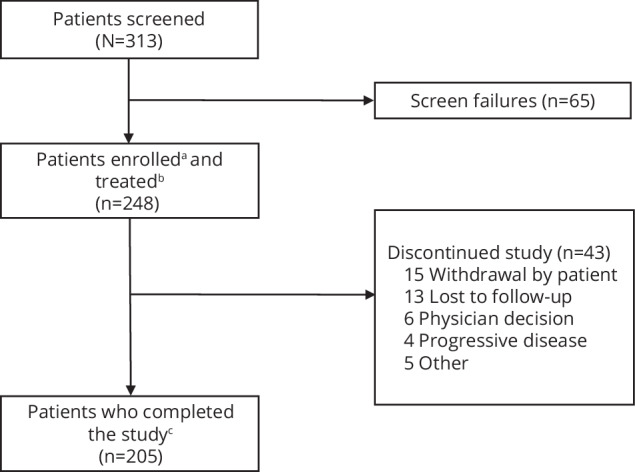
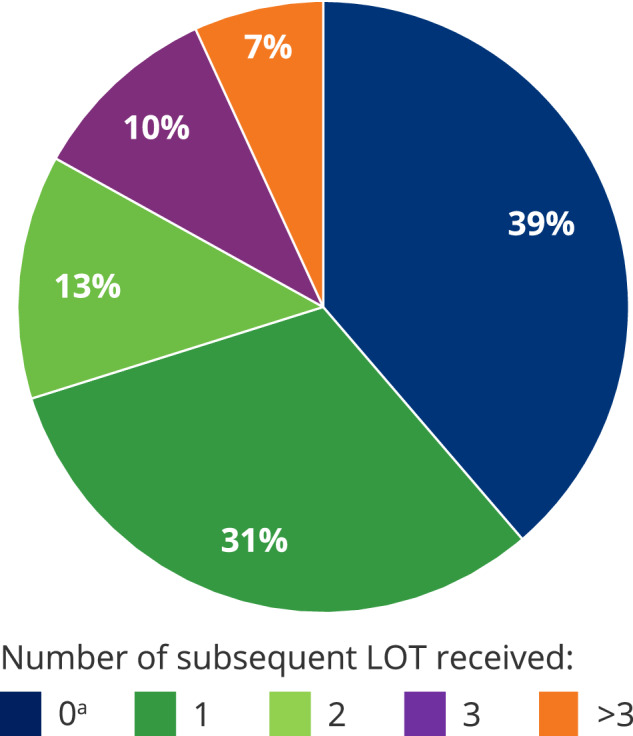
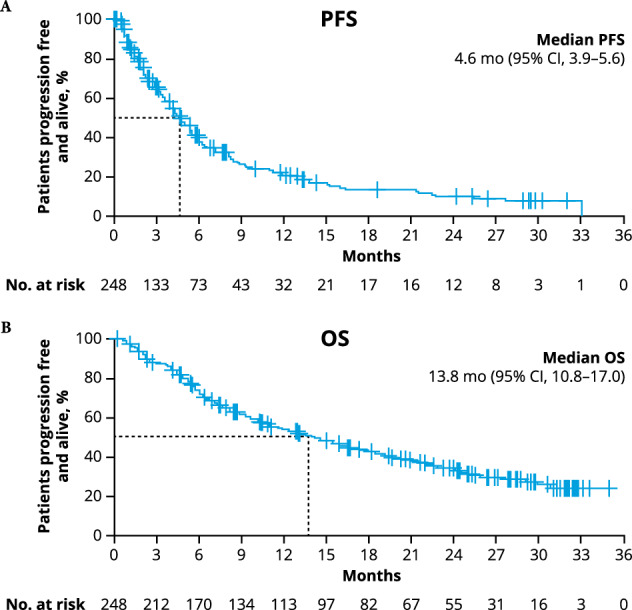
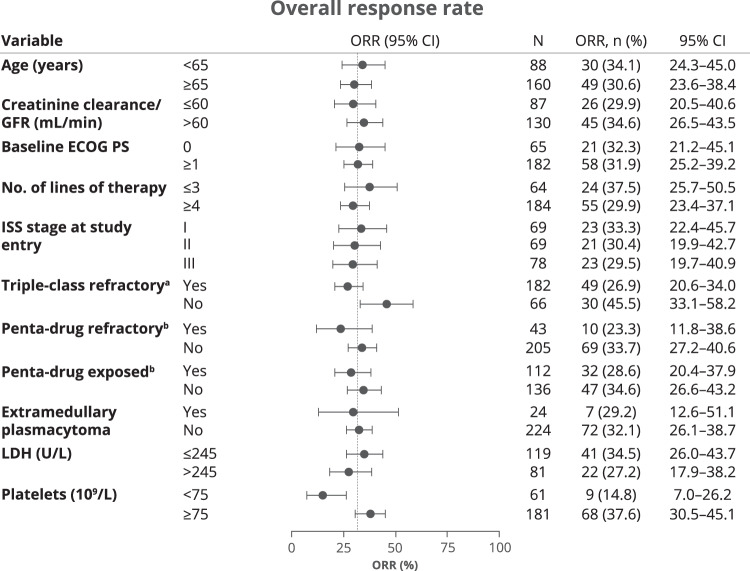
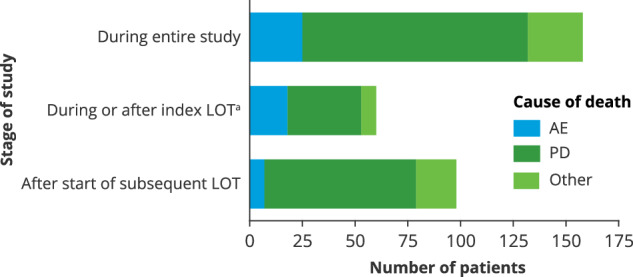
Treatment of relapsed/refractory multiple myeloma (RRMM) is challenging as patients exhaust all available therapies and the disease becomes refractory to standard drug classes. Here we report the final results of LocoMMotion, the first prospective study of real-world clinical practice (RWCP) in triple-class exposed (TCE) patients with RRMM, with a median follow-up of 26.4 months (range, 0.1-35.0). Patients (N = 248) had received median 4 prior LOT (range, 2-13) at enrollment. 91 unique regimens were used in index LOT. Overall response rate was 31.9% (95% CI, 26.1-38.0), median progression-free survival (PFS) was 4.6 months (95% CI, 3.9-5.6) and median overall survival was 13.8 months (95% CI, 10.8-17.0). 152 patients (61.3%) had subsequent LOTs with 134 unique regimens, of which 78 were used in first subsequent LOT. Median PFS2 (from start of study through first subsequent LOT) was 10.8 months (95% CI, 8.4-13.0). 158 patients died on study, 67.7% due to progressive disease. Additional subgroup analyses and long-term safety summaries are reported. The high number of RWCP treatment regimens utilized and poor clinical outcomes confirm a lack of standardized treatment for TCE patients with RRMM, highlighting the need for new treatments with novel mechanisms.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: M-VM has received honoraria from or served on the board of directors/advisory committees for AbbVie, Adaptive Biotechnologies, Amgen, BMS/Celgene, GSK, Janssen, Oncopeptides, Pfizer, Regeneron, Roche, Sanofi, Seagen, and Takeda. KW has served as a consultant and received honoraria from Adaptive Biotechnologies, Karyopharm, and Takeda; has received honoraria from Roche; and has received honoraria and served as a member on boards of directors and/or advisory committees for Amgen, BMS, Celgene, GSK, Janssen, Oncopeptides, and Sanofi. VDS has served on an advisory board or speakers’ bureaus and received honoraria from AbbVie, Alexion, AOP Health, argenx, BMS, GSK, Grifols, Leo Pharma, Novartis, Novo Nordisk, Sanofi, SOBI, and Takeda. HG has served as a consultant for Amgen, Novartis, and Takeda; has served as a consultant and received honoraria, grants, and/or provision of investigational medicinal product and research funding from Amgen, BMS, Celgene, Chugai, Janssen, and Sanofi; has received research funding from Incyte, Molecular Partners, MSD, Mundipharma, and Novartis; and has received other grants from Dietmer Hopp Foundation. MD has received honoraria from Amgen, BMS, GSK, and Janssen; and has served on the speakers’ bureau for Janssen. MM has received honoraria from Adaptive Biotech, Amgen, Astellas, BMS, Gilead, Novartis, Pfizer, and Takeda; and has received honoraria/research funding from Celgene and Sanofi. JL-H has no relationships to disclose. DD is an employee/consultant/honoraria/member of board of directors/advisory committees for Janssen Cilag; and a member of the board of directors/advisory committees/received research funding from Celgene. EA has no relationships to disclose. LV has served on the advisory board of BMS, Janssen, and Takeda. AP has received honoraria from or has served in a consulting/advisory role for AbbVie, Amgen, BMS, Janssen, Pfizer, Sanofi, and Takeda. RB has received honoraria/research funding from Allogene, BMS, Gilead, Janssen, and Servier. NWCJvdD has received research funding from AbbVie, Amgen, BMS, Celgene, Cellectis, Janssen Pharmaceuticals, and Novartis; and has served in a consulting/advisory role for Adaptive, Amgen, Bayer, BMS, Celgene, Janssen, Novartis, Pfizer, Roche, Sanofi, Servier, and Takeda. EMO has received honoraria from or has served in a consulting/advisory role for AbbVie, Amgen, BMS, GSK, Janssen, Karyopharm, Menarini, Oncopeptides, Pfizer, Sanofi, and Takeda. TR is a former Janssen employee. JMS is a Janssen employee. SK is a Janssen employee. IH is a Janssen employee. VS is a Janssen employee. LM is a Janssen employee. JB is a Janssen employee. OCF is an employee of Legend Biotech USA Inc. HE has received research funding or honoraria and has served in a consulting/advisory role for Amgen, BMS/Celgene, GSK, Janssen, and Sanofi. PM has received honoraria and/or served on advisory boards for AbbVie, Amgen, Celgene, Janssen, Sanofi, and Takeda.
Figures
References
-
- Rodríguez-Lobato LG, Pereira A, Fernández de Larrea C, Cibeira MT, Tovar N, Jiménez-Segura R, et al. Real-world data on survival improvement in patients with multiple myeloma treated at a single institution over a 45-year period. Br J Haematol. 2022;196:649–59. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
