

Epcoritamab in relapsed/refractory large B-cell lymphoma: 2-year follow-up from the pivotal EPCORE NHL-1 trial
- PMID: 39322711
- PMCID: PMC11588654
- DOI: 10.1038/s41375-024-02410-8
Epcoritamab in relapsed/refractory large B-cell lymphoma: 2-year follow-up from the pivotal EPCORE NHL-1 trial
Abstract
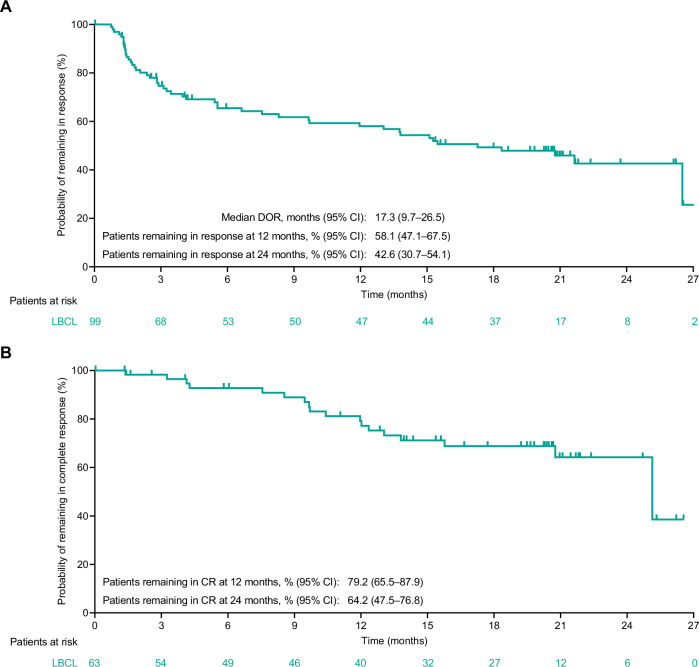
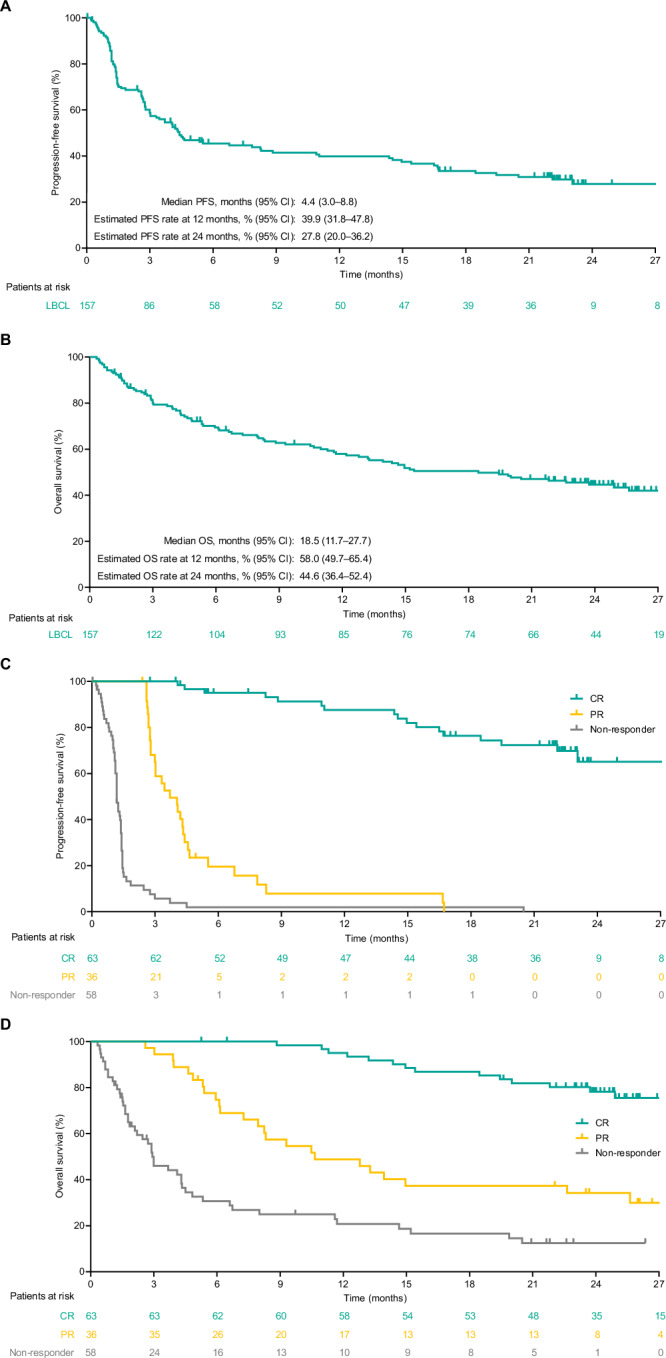
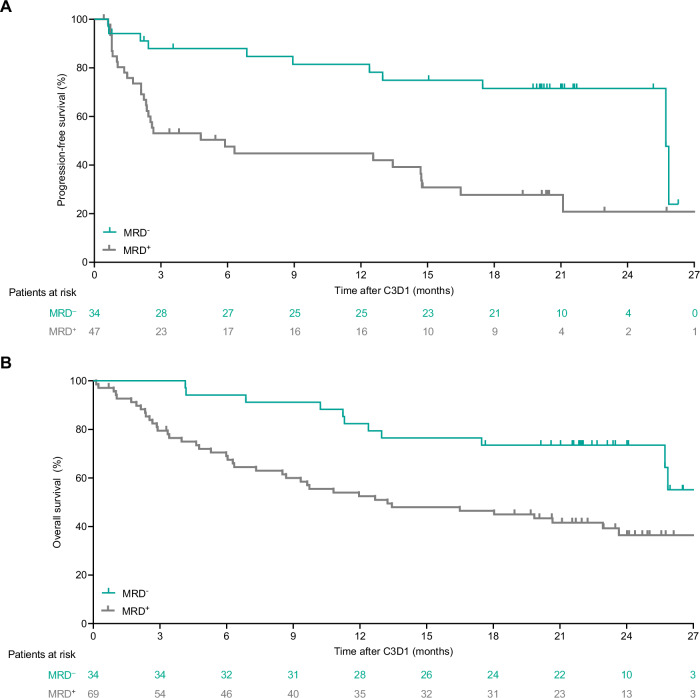
Primary results (median follow-up, 10.7 months) from the pivotal EPCORE® NHL-1 study in relapsed or refractory (R/R) large B-cell lymphoma (LBCL) demonstrated deep, durable responses with epcoritamab, a CD3xCD20 bispecific antibody, when used as monotherapy. We report long-term efficacy and safety results in patients with LBCL (N = 157; 25.1-month median follow-up). As of April 21, 2023, overall response rate was 63.1% and complete response (CR) rate was 40.1%. Estimated 24-month progression-free survival (PFS) and overall survival (OS) rates were 27.8% and 44.6%, respectively. An estimated 64.2% of complete responders remained in CR at 24 months. Estimated 24-month PFS and OS rates among complete responders were 65.1% and 78.2%, respectively. Of 119 minimal residual disease (MRD)-evaluable patients, 45.4% had MRD negativity, which correlated with longer PFS and OS. CR rates were generally consistent across predefined subgroups: 36% prior chimeric antigen receptor (CAR) T-cell therapy, 32% primary refractory disease, and 37% International Prognostic Index ≥3. The most common treatment-emergent adverse events were cytokine release syndrome (51.0%), pyrexia (24.8%), fatigue (24.2%), and neutropenia (23.6%). These results underscore the long-term benefit of epcoritamab for treating R/R LBCL with deep responses across subgroups, including patients with hard-to-treat disease and expected poor prognosis (ClinicalTrials.gov Registration: NCT03625037).
© 2024. The Author(s).
Conflict of interest statement
Competing interests: CT reports research funding from BMS, Hospira, and Roche; consulting role for AbbVie, Amgen, BMS, Cellectis, Gilead Sciences, Kite, Novartis, and Roche; honoraria from AbbVie, Amgen, Bayer, Cellectis, Gilead Sciences, Incyte, Janssen, Kite, Novartis, and Takeda; membership on an entity’s board of directors or advisory committees at AbbVie, Amgen, BMS, Cellectis, Gilead Sciences, Incyte, Janssen, Kite, Novartis, Roche, and Takeda; and travel expenses from AbbVie, Amgen, BMS, Cellectis, Gilead Sciences, Kite, Novartis, and Roche. YHK reports consulting/advisory role for AbbVie and ADC Therapeutics; travel expenses from Roche/Genentech; and research funding from AbbVie, AstraZeneca, Lilly/Loxo, Merck, Roche/Genentech, and Xencor. HG reports consulting role for Gilead and Roche; and honoraria from AbbVie, BMS, Gilead, and Roche. CYC reports consulting/advisory roles and honoraria from Roche, Janssen, Gilead, AstraZeneca, Lilly, BeiGene, Menarini, Dizal, AbbVie, Genmab, Sobi, BMS, and Regeneron; research funding from BMS, Roche, AbbVie, MSD, and Lilly; speakers bureau for Janssen, AstraZeneca, BeiGene, Genmab, AbbVie, and Roche; and travel expenses from Lilly and BeiGene. MRC reports consulting role for AbbVie, Janssen, Gilead, AstraZeneca, Genmab, and Incyte; advisory role for AbbVie, Janssen, Gilead, and Genmab; and travel expenses from AbbVie, Janssen, AstraZeneca, Genmab, Roche, and Pfizer. DC reports research grants (paid to institution, Royal Marsden Hospital) from MedImmune/AstraZeneca, Clovis, Lilly, 4SC, Bayer, BMS, and Roche. WJ reports research funding and consulting role for AbbVie and Roche. YRD reports no conflicts of interest. RG reports honoraria from MSD, Otsuka, Novartis, Astellas, Janssen, AbbVie, and Takeda. DJL reports consulting/advisory role for Janssen, Lilly, Roche, BeiGene, and Kite. TMK reports consulting for Amgen, AstraZeneca/MedImmune, Boryung, Daiichi Sankyo, F. Hoffmann-La Roche Ltd/Genentech, HK inno.N, Janssen, Novartis, Regeneron, Samsung Bioepis, Takeda, and Yuhan; honoraria from Amgen, AstraZeneca/MedImmune, IMBdx, Janssen, and Takeda; and membership on an entity’s board of directors or advisory committees at Amgen, BeiGene, Janssen, Novartis, Regeneron, Samsung Bioepis, and Takeda. MvdP reports no conflicts of interest. MLP reports no conflicts of interest. TF reports consulting role for AbbVie, AstraZeneca, Epizyme, Genmab, Gilead/Kite, Karyopharm, and Takeda; and consulting role/speakers bureau for Seagen. KML reports membership on the Epcoritamab Global Council for Genmab; consulting/advisory role for AbbVie, BeiGene, BMS, Genmab, Kite/Gilead, and Roche; speakers bureau for AbbVie and BMS; research funding (paid to institution) from AbbVie, ADC Therapeutics, AstraZeneca, BeiGene, BMS, CellCentric, Genmab, Janssen, Kite/Gilead, MorphoSys, MSD, Nurix, Regeneron, Roche, Step Pharma, and Viracta; and travel expenses from BMS. AS reports consulting role for Takeda, BMS, Novartis, Janssen, MSD, Amgen, GSK, Sanofi, Kite, and Mundipharma; honoraria from Takeda, BMS, Novartis, Janssen, MSD, Amgen, GSK, Sanofi, and Kite; membership on an entity’s board of directors or advisory committees for Takeda, BMS, Novartis, Janssen, Amgen, Bluebird, Sanofi, and Kite; travel expenses from Takeda, BMS, and Roche; research funding from Takeda; and speakers bureau for Takeda, BMS, Novartis, Janssen, MSD, Amgen, GSK, Sanofi, and Kite. MH reports scientific advisory boards for AbbVie, BMS, Genmab, Janssen, Roche, and Takeda; and research support (paid to institution) from BMS, Genentech, Genmab, Incyte, Janssen, Novartis, Roche, and Takeda. MHD reports employment with AbbVie. NK reports employment with Genmab. DS reports employment with Genmab. TM reports employment with Genmab. MS reports employment with Genmab. TP reports consulting/advisory role for Pfizer/Seagen, Pharmacyclics, Incyte, Genentech, Bayer, Gilead Sciences, Curis, Kite/Gilead, BMS, Genmab, TG Therapeutics, and ADC Therapeutics; honoraria from Pfizer/Seagen and Lymphoma & Myeloma Connect; research funding from AbbVie, Pharmacyclics/Janssen, and Bayer; and is a scholar in the Clinical Research of The Leukemia & Lymphoma Society. PJL reports research grants from Takeda and Servier; advisory honoraria from BMS, Roche, Takeda, Genmab, AbbVie, Incyte, Regeneron, and Sandoz; and consultancy honoraria from Y-mAbs Therapeutics. Ethics approval and consent to participate: The trial was conducted in accordance with regulatory requirements, International Council for Harmonization Good Clinical Practice Guidelines, and the Declaration of Helsinki. The study protocol was approved by site-specific Institutional Review Boards and/or Institutional or Central Ethics Committees (Central Ethics Committee: Hôpital Saint-Antoine Comité de Protection des Personnes [CPP] Ile de France V; Paris, France; 2017-001748-36), and all patients provided written informed consent.
Figures
Similar articles
-
Efficacy and safety of epcoritamab in Japanese patients with relapsed or refractory diffuse large B-cell lymphoma: 3-year follow-up from the EPCORE NHL-3 trial.Int J Clin Oncol. 2025 Aug;30(8):1631-1640. doi: 10.1007/s10147-025-02788-0. Epub 2025 May 28. Int J Clin Oncol. 2025. PMID: 40434509 Free PMC article. Clinical Trial.
-
Epcoritamab plus GemOx in transplant-ineligible relapsed/refractory DLBCL: results from the EPCORE NHL-2 trial.Blood. 2025 Apr 10;145(15):1621-1631. doi: 10.1182/blood.2024026830. Blood. 2025. PMID: 39792928 Free PMC article. Clinical Trial.
-
Epcoritamab, a Novel, Subcutaneous CD3xCD20 Bispecific T-Cell-Engaging Antibody, in Relapsed or Refractory Large B-Cell Lymphoma: Dose Expansion in a Phase I/II Trial.J Clin Oncol. 2023 Apr 20;41(12):2238-2247. doi: 10.1200/JCO.22.01725. Epub 2022 Dec 22. J Clin Oncol. 2023. PMID: 36548927 Free PMC article. Clinical Trial.
-
Rituximab: a review of its use in non-Hodgkin's lymphoma and chronic lymphocytic leukaemia.Drugs. 2003;63(8):803-43. doi: 10.2165/00003495-200363080-00005. Drugs. 2003. PMID: 12662126 Review.
-
The value of bispecific antibodies in relapsed and refractory DLBCL.Leuk Lymphoma. 2024 Jun;65(6):720-735. doi: 10.1080/10428194.2024.2323085. Epub 2024 Mar 7. Leuk Lymphoma. 2024. PMID: 38454535 Review.
Cited by
-
Infectious Complications in Patients with B-Cell Non-Hodgkin Lymphoma Treated with Bispecific Antibodies.Cancers (Basel). 2025 Jul 22;17(15):2426. doi: 10.3390/cancers17152426. Cancers (Basel). 2025. PMID: 40805129 Free PMC article. Review.
-
Allogeneic CAR-engineered cellular therapy for relapsed and refractory large B cell lymphoma: a systematic review and meta-analysis.Front Immunol. 2025 Jul 8;16:1585556. doi: 10.3389/fimmu.2025.1585556. eCollection 2025. Front Immunol. 2025. PMID: 40698082 Free PMC article.
-
The Current State of Bispecific Antibodies and T-Cell Directed Therapy in NHL.Cancers (Basel). 2025 Mar 31;17(7):1192. doi: 10.3390/cancers17071192. Cancers (Basel). 2025. PMID: 40227768 Free PMC article. Review.
-
Optimal Use of Bispecific Antibodies for the Treatment of Diffuse Large B-Cell Lymphoma in Canada.Curr Oncol. 2025 Feb 28;32(3):142. doi: 10.3390/curroncol32030142. Curr Oncol. 2025. PMID: 40136346 Free PMC article. Review.
-
Targeting myeloid cells for hematological malignancies: the present and future.Biomark Res. 2025 Apr 10;13(1):59. doi: 10.1186/s40364-025-00775-1. Biomark Res. 2025. PMID: 40205623 Free PMC article. Review.
References
-
- Wienand K, Chapuy B. Molecular classification of aggressive lymphomas-past, present, future. Hematol Oncol. 2021;39:24–30. - PubMed
-
- Jakobsen LH, Bøgsted M, Brown PN, Arboe B, Jørgensen J, Larsen TS, et al. Minimal loss of lifetime for patients with diffuse large B-cell lymphoma in remission and event free 24 months after treatment: a Danish population-based study. J Clin Oncol. 2017;35:778–84. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
