

The Pupillary Light-Off Reflex in Acute Disorders of Consciousness
- PMID: 39322845
- PMCID: PMC11950040
- DOI: 10.1007/s12028-024-02133-9
The Pupillary Light-Off Reflex in Acute Disorders of Consciousness
Abstract
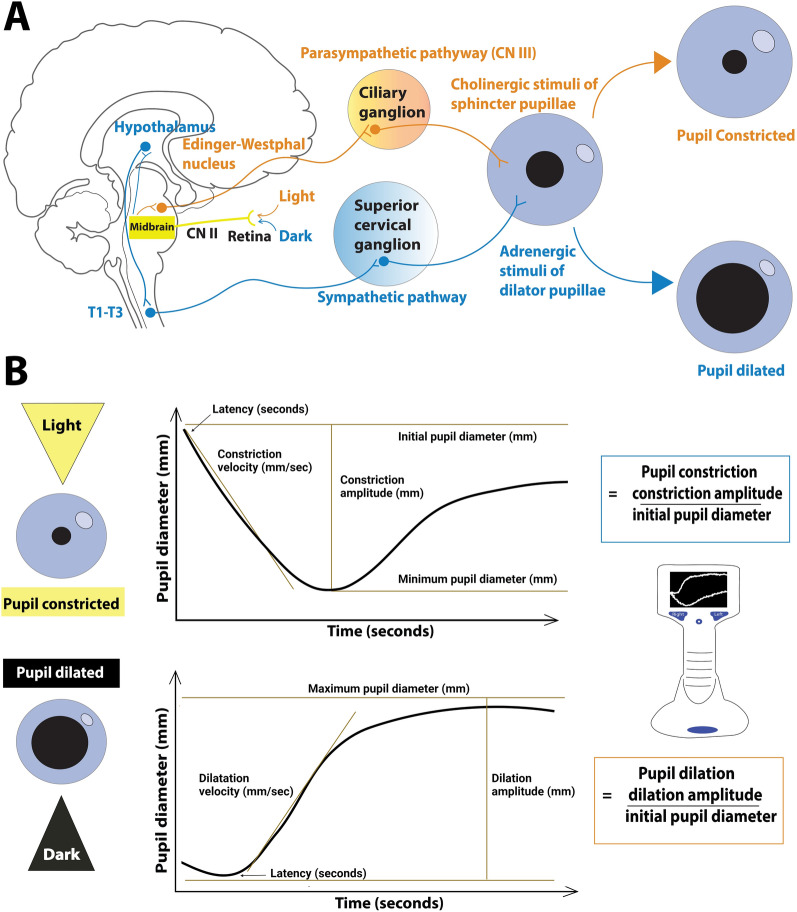
Background: In intensive care patients with disorders of consciousness, the pupillary light reflex is a measure of pupillary parasympathetic function. By contrast, the pupillary light-off reflex leads to pupil dilation in response to an abrupt change from light to darkness ("light-off") and reflects combined parasympathetic and sympathetic pupillary function. To our knowledge, this reflex has not been systematically investigated in patients with disorders of consciousness. We hypothesized that the pupillary light-off reflex correlates with consciousness levels after acute brain injury.
Methods: From November 2022 to March 2023, we enrolled 100 study participants: 25 clinically unresponsive (coma or unresponsive wakefulness syndrome) and 25 clinically low-responsive (minimally conscious state or better) patients from the intensive care units of a tertiary referral center, and 50 age-matched and sex-matched healthy controls. Exclusion criteria were active or chronic eye disease. We used automated pupillometry to assess the pupillary light-off reflex and the pupillary light reflex of both eyes under scotopic conditions in all study participants.
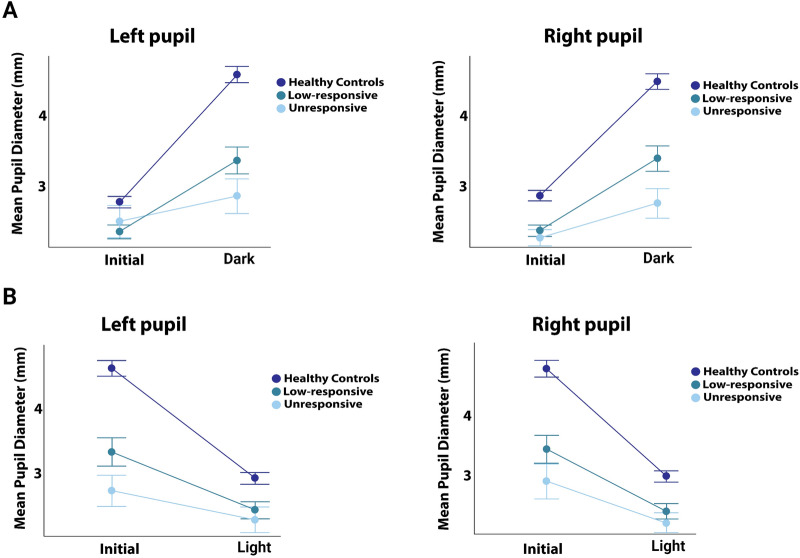
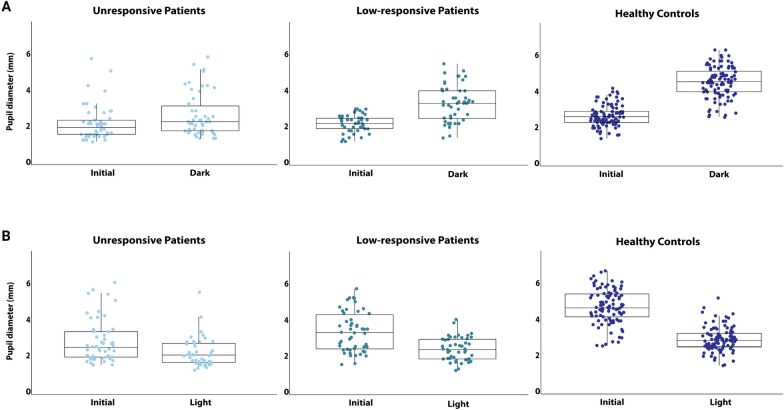
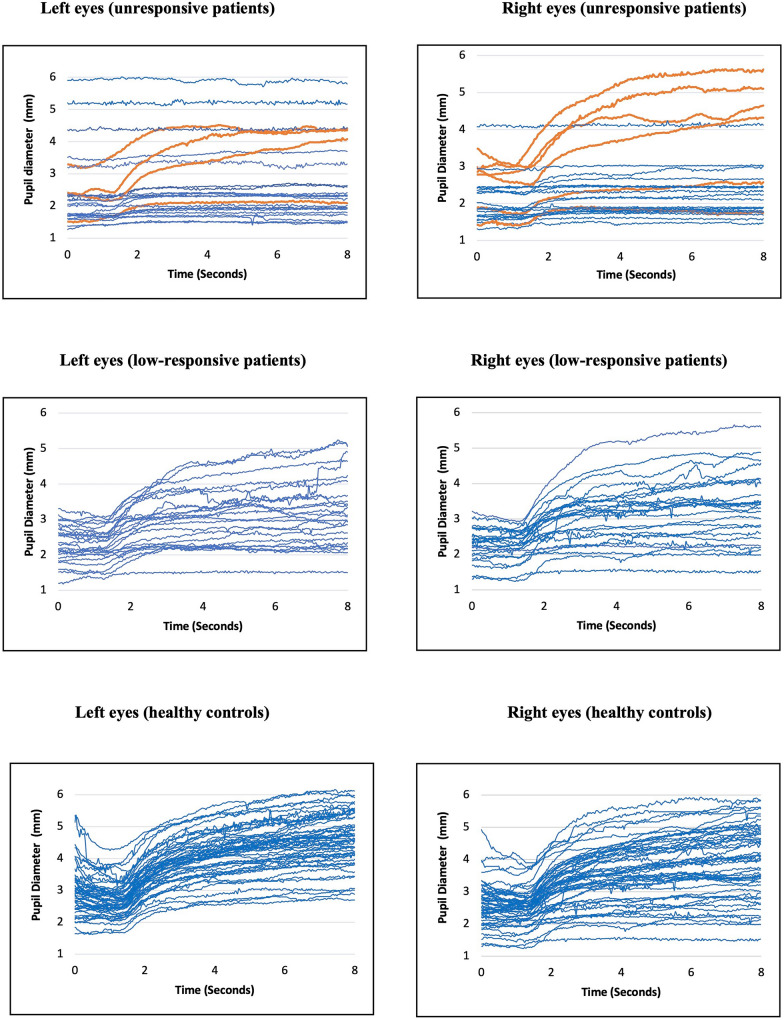
Results: The pupillary light-off reflex was strongly correlated with consciousness levels (r = 0.62, p < 0.001), the increase in pupillary diameters being smallest in unresponsive patients (mean ± standard deviation 20% ± 21%), followed by low-responsive patients (mean ± standard deviation 47% ± 26%) and healthy controls (mean ± standard deviation 67% ± 17%; p < 0.001). Similar yet less pronounced patterns were observed for the pupillary light reflex. Twenty-one of 25 (84%) unresponsive patients had preserved pupillary light reflexes, but only seven (28%) had fully preserved pupillary light-off reflexes (p < 0.0001). Of these 7 patients, five (71%) regained awareness.
Conclusions: The pupillary light-off reflex may be more sensitive to consciousness levels than the pupillary light reflex. The clinical implications of this finding seem worthy of further investigation, particularly regarding possible benefits for neuromonitoring and prognostication after brain injury.
Keywords: Brain injury; Coma; Consciousness; Neuromonitoring; Prognostication; Pupillometry.
© 2024. The Author(s).
Conflict of interest statement
Conflicts of interest: The authors report no competing interests. Ethical approval/informed consent: The study adhered to the Declaration of Helsinki and received approval from the regional Danish Research Ethics Committee (H-21022096). Ethical guidelines were adhered to, and we indicate ethical approvals (institutional review board) and use of informed consent, and we confirm the use of an appropriate reporting checklist.
Figures
References
-
- Loewenfeldt I. The pupil: anatomy, physiology, and clinical applications. 2nd ed. Oxford: Butterworth-Heinemann; 1999.
-
- Hunyor AP. Reflexes and the eye. Aust N Z J Ophthalmol. 1994;22:155–9. - PubMed
-
- Cherng Y-G, Crevecoeur F, Wang C-A. Effects of pupillary light and darkness reflex on the generation of pro- and anti-saccades. Eur J Neurosci. 2021;53:1769–82. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
