

Early economic evaluation of magnetic resonance imaging for prostate cancer detection in primary care
- PMID: 39323927
- PMCID: PMC11420105
- DOI: 10.1002/bco2.409
Early economic evaluation of magnetic resonance imaging for prostate cancer detection in primary care
Erratum in
-
Erratum.BJUI Compass. 2024 Dec 30;5(12):1324-1329. doi: 10.1002/bco2.482. eCollection 2024 Dec. BJUI Compass. 2024. PMID: 39744071 Free PMC article.
Abstract
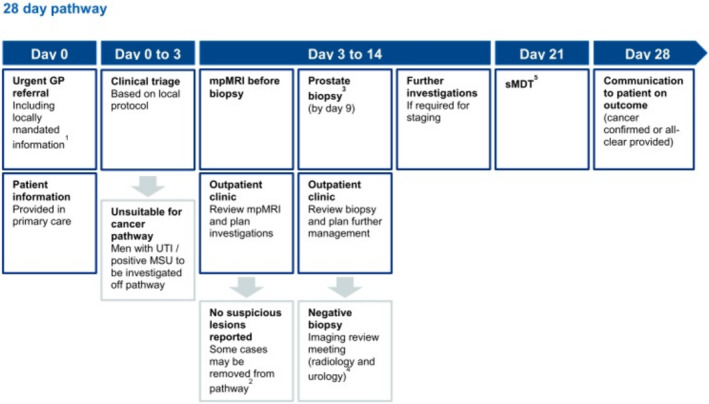
Objectives: To explore the potential impacts of incorporating prebiopsy magnetic resonance imaging into primary care as a triage test within the prostate cancer diagnostic pathway.
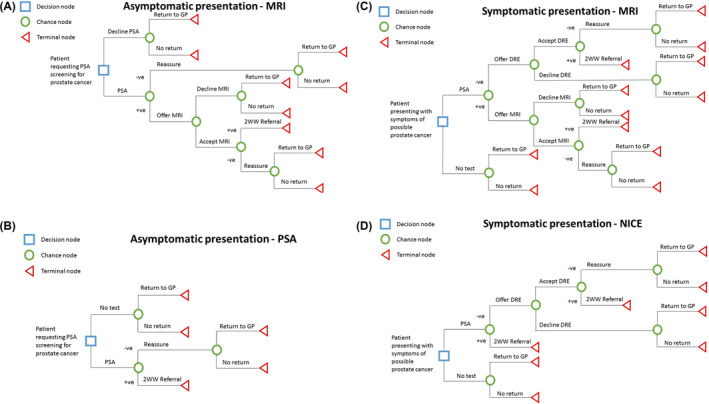
Subjects and methods: Decision analytic modelling with decision trees was utilised for this early economic evaluation. A conceptual model was developed reflecting the common primary care routes to diagnosis for prostate cancer: opportunistic, asymptomatic prostate-specific antigen (PSA) screening or symptomatic presentation. The use of multiparametric MRI (mpMRI) or biparametric MRI (bpMRI) as a primary care triage test following an elevated PSA result was evaluated. A health system perspective was adopted with a time horizon of 12 months. Health effects were expressed in terms of utilities drawn from the literature. The primary outcome was prostate cancer diagnosis. Evidence used to inform the model was drawn from published primary studies, systematic reviews, and secondary analyses of primary and secondary care datasets.
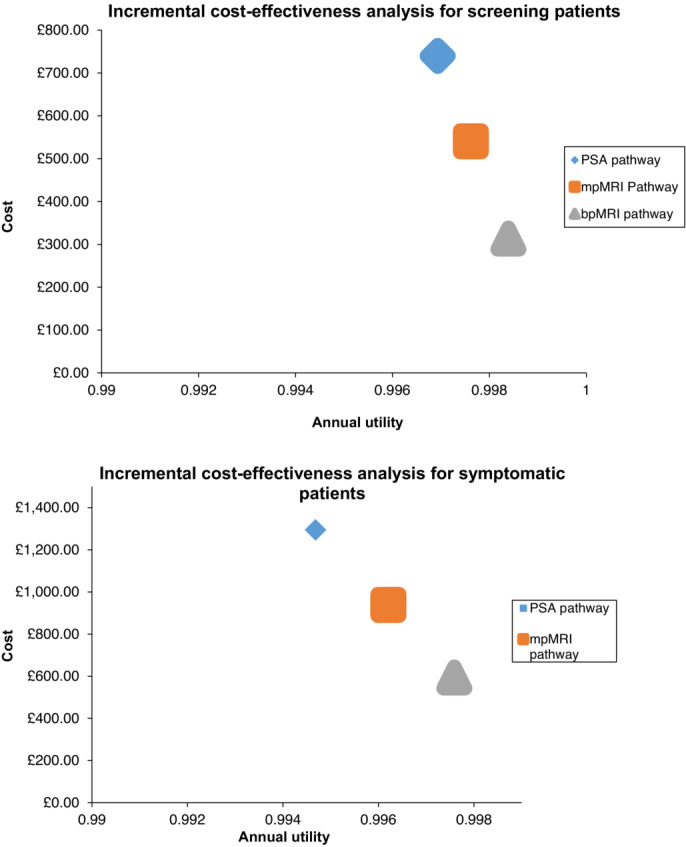
Results: Base case analysis showed that the PSA pathway was dominated by both mpMRI- and bpMRI-based pathways for patients undergoing opportunistic screening and symptomatic assessment. bpMRI pathways had greater improvement in cost and utility than mpMRI pathways in both clinical scenarios. Significantly more MRI scans would be performed using the modelled approach (66 626 scans vs. 37 456 scans per 100 000 patients per annum), with fewer subsequent urgent suspected cancer referrals for both mpMRI (38% reduction for screening and symptomatic patients) and bpMRI (72% reduction for screening; 71% for symptomatic) pathways, and a small increase in number of missed cancer diagnoses. Deterministic sensitivity analyses, varying each parameter to its upper and lower 95% confidence intervals, showed no significant change in the dominance of the MRI-based prostate cancer diagnostic pathways.
Conclusion: Using prostate MRI as a second-level triage test for suspected prostate cancer in primary care could reduce health service costs without a detrimental effect on patient utility.
Keywords: Prostate cancer; bpMRI; diagnosis; early economic evaluation; mpMRI; primary care.
© 2024 The Author(s). BJUI Compass published by John Wiley & Sons Ltd on behalf of BJU International Company.
Conflict of interest statement
The authors have no declarations of interest to make in relation to this study.
Figures
References
-
- Ahmed HU, Bosaily AE‐S, Brown LC, Gabe R, Kaplan R, Parmar MK, et al. Diagnostic accuracy of multi‐parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet. 2017;380:1–8. - PubMed
-
- England N. Implementing a timed prostate cancer diagnostic pathway NHS; 2018.
-
- NICE . Prostate Cancer: Diagnosis and Management. ng131 London: National Institute for Health and Care Excellence; 2019.
-
- Loeb S, Vellekoop A, Ahmed HU, Catto J, Emberton M, Nam R, et al. Systematic review of complications of prostate biopsy. Eur Urol. 2013;64(6):876–892. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous