

Formalized peer referral to HIV pre-exposure prophylaxis supported with self-testing: a mixed-methods pilot study among young Kenyan women
- PMID: 39324163
- PMCID: PMC11422135
- DOI: 10.3389/fpubh.2024.1428609
Formalized peer referral to HIV pre-exposure prophylaxis supported with self-testing: a mixed-methods pilot study among young Kenyan women
Abstract
Background: The uptake of daily oral HIV pre-exposure prophylaxis (PrEP)-a highly effective intervention-remains low among African adolescent girls and young women (AGYW) who could benefit. AGYW who initiate PrEP often do so through informal peer referral, which may be enhanced with formalized peer referral and peer-delivered HIV self-testing (HIVST). To understand the feasibility of this PrEP referral model among AGYW, we conducted a pilot study in Kenya.
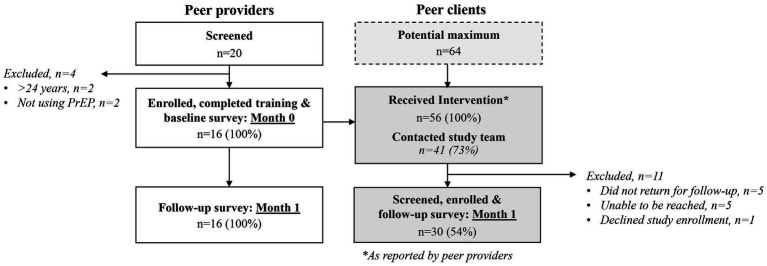
Method: From March to May 2022, we recruited AGYW (≥16-24 years) using PrEP (i.e., "peer providers") from public healthcare clinics in Kiambu County and trained them on HIV prevention, HIVST use, and peer-supported linkage to clinic-based HIV services. Following training, peer providers received eight HIVST kits and were encouraged to refer four peers (i.e., "peer clients") to PrEP. We completed surveys with peer providers and clients one month following intervention delivery to assess PrEP initiation among peer clients. Later, we conducted focus group discussions (FGDs) with peer providers and clients to identify factors that facilitated or challenged intervention outcomes.
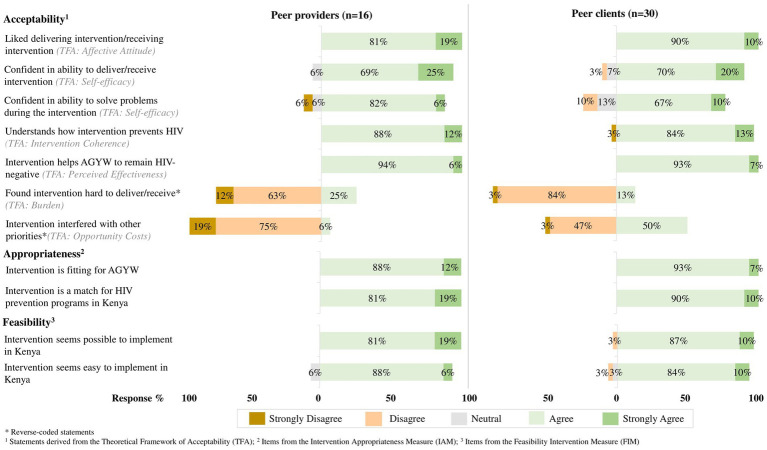
Results: We trained 16 peer providers (median age: 23 years, IQR 21-24) who reported delivering the intervention to 56 peer clients; 30 peer clients (median age: 21 years, IQR 19-22) contacted the study team and were enrolled. Most of the enrolled peer clients reported behaviors associated with HIV risk (e.g., condomless sex; 80%, 24/30) and were PrEP-naïve (87%, 26/30). At one-month, PrEP initiation among eligible PrEP-naïve peer clients was high, as reported by providers (78%, 43/55) and clients (85%, 22/26); recent HIVST use was also high among peer clients (provider report: 95%, 53/56; client report: 97%, 29/30). In the FGDs, participants reported that intervention outcomes were facilitated by close preexisting relationships, HIVST assistance, and being escorted to clinic-based HIV services by peer providers; intervention barriers included conflicting priorities and limited HIVST experience.
Conclusion: A formalized model of peer referral with HIVST delivery supported PrEP initiation among Kenyan AGYW. These findings demonstrate the potential for peer-delivered interventions to engage AGYW in HIV prevention services; however, more research is needed on the effectiveness and sustainability of this approach at scale.
Keywords: AGYW; HIV self-test; peer delivery; pre-exposure prophylaxis; sub-Saharan Africa.
Copyright © 2024 McGowan, Wairimu, Reedy, Mogere, Culquichicon, Njeru, Malen, Jahn, Bärnighausen, Roche, Ngure and Ortblad.
Conflict of interest statement
PM is currently an employee of Novartis following completion of the presented research. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
Similar articles
-
Peer PrEP referral + HIV self-test delivery for PrEP initiation among young Kenyan women: study protocol for a hybrid cluster-randomized controlled trial.Trials. 2023 Nov 4;24(1):705. doi: 10.1186/s13063-023-07734-x. Trials. 2023. PMID: 37925450 Free PMC article.
-
Assessing young Kenyan women's willingness to engage in a peer-delivered HIV self-testing and referral model for PrEP initiation: A qualitative formative research study.Front Public Health. 2022 Oct 6;10:932948. doi: 10.3389/fpubh.2022.932948. eCollection 2022. Front Public Health. 2022. PMID: 36276357 Free PMC article.
-
Feasibility and acceptability of peer-delivered HIV self-testing and PrEP for young women in Kampala, Uganda.BMC Public Health. 2023 Jun 16;23(1):1163. doi: 10.1186/s12889-023-16081-0. BMC Public Health. 2023. PMID: 37322510 Free PMC article.
-
PrEP Uptake and Utilisation Among Adolescent Girls and Young Women in Sub-Saharan Africa: A Scoping Review.AIDS Behav. 2025 Jun;29(6):1876-1896. doi: 10.1007/s10461-025-04656-4. Epub 2025 Feb 28. AIDS Behav. 2025. PMID: 40021551 Free PMC article.
-
HIV pre-exposure prophylaxis for adolescent girls and young women in Africa: from efficacy trials to delivery.J Int AIDS Soc. 2019 Jul;22 Suppl 4(Suppl Suppl 4):e25298. doi: 10.1002/jia2.25298. J Int AIDS Soc. 2019. PMID: 31328444 Free PMC article. Review.
Cited by
-
Examining concordance of sexual-related factors and PrEP eligibility with HIV risk perception among adolescent girls and young women: cross-sectional insights from DREAMS sites in Kenya, Malawi, and Zambia.BMC Public Health. 2024 Oct 12;24(1):2793. doi: 10.1186/s12889-024-20276-4. BMC Public Health. 2024. PMID: 39395932 Free PMC article.
References
-
- UNAIDS . Kenya launches self-test kits and PrEP [internet]. Geneva, Switzerland: UNAIDS; (2017). Available at: https://www.unaids.org/en/resources/presscentre/featurestories/2017/may/... (Accessed November 25, 2022).
-
- National AIDS & STI Control Program . Framework for the implementation of pre-exposure prophylaxis of HIV in Kenya. Nairobi, Kenya: NASCOP; (2017). 84 p.
-
- National AIDS & STI Control Program . Kenya population-based HIV impact assessment: KENPHIA 2018. Nairobi, Kenya: NASCOP; (2022). 322 p.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous