

Longitudinal associations between exercise and biomarkers in autosomal dominant Alzheimer's disease
- PMID: 39324510
- PMCID: PMC11567864
- DOI: 10.1002/alz.14270
Longitudinal associations between exercise and biomarkers in autosomal dominant Alzheimer's disease
Abstract
Introduction: We investigated longitudinal associations between self-reported exercise and Alzheimer's disease (AD)-related biomarkers in individuals with autosomal dominant AD (ADAD) mutations.
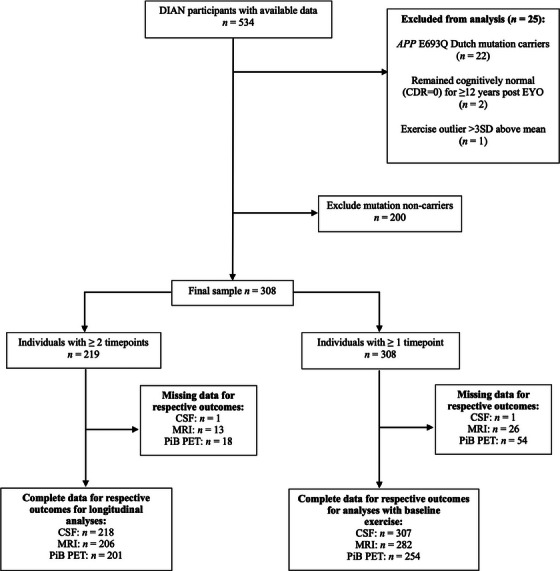
Methods: Participants were 308 ADAD mutation carriers aged 39.7 ± 10.8 years from the Dominantly Inherited Alzheimer's Network. Weekly exercise volume was measured via questionnaire and associations with brain volume (magnetic resonance imaging), cerebrospinal fluid biomarkers, and brain amyloid beta (Aβ) measured by positron emission tomography were investigated.
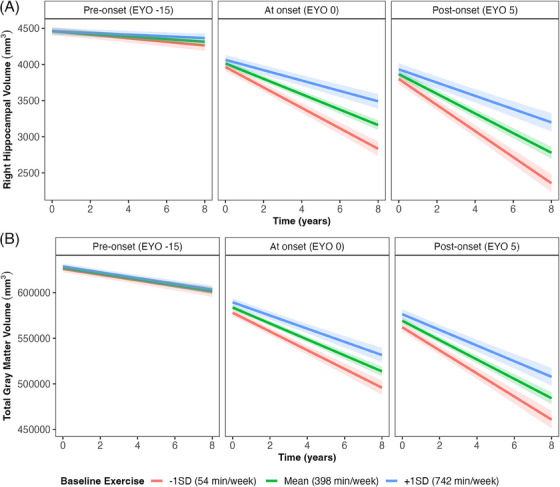
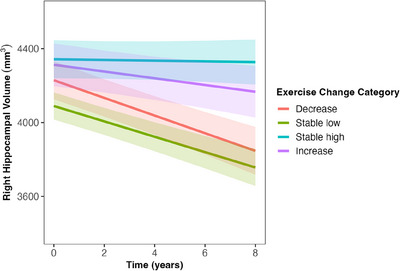
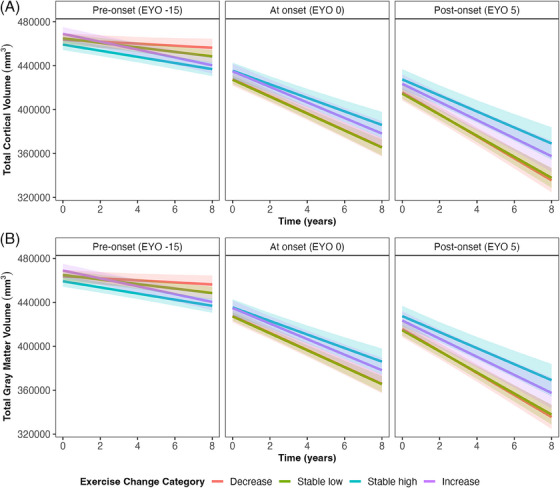
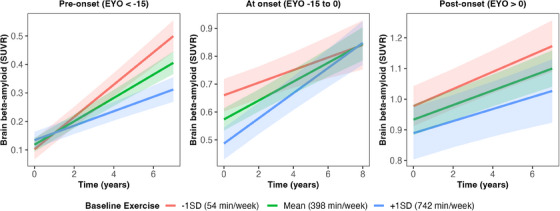
Results: Greater volume of weekly exercise at baseline was associated with slower accumulation of brain Aβ at preclinical disease stages β = -0.16 [-0.23 to -0.08], and a slower decline in multiple brain regions including hippocampal volume β = 0.06 [0.03 to 0.08].
Discussion: Exercise is associated with more favorable profiles of AD-related biomarkers in individuals with ADAD mutations. Exercise may have therapeutic potential for delaying the onset of AD; however, randomized controlled trials are vital to determine a causal relationship before a clinical recommendation of exercise is implemented.
Highlights: Greater self-reported weekly exercise predicts slower declines in brain volume in autosomal dominant Alzheimer's disease (ADAD). Greater self-reported weekly exercise predicts slower accumulation of brain amyloid beta in ADAD. Associations varied depending on closeness to estimated symptom onset.
Keywords: Alzheimer's disease; exercise; magnetic resonance imaging; physical activity; positron emission tomography.
© 2024 The Author(s). Alzheimer's & Dementia published by Wiley Periodicals LLC on behalf of Alzheimer's Association.
Conflict of interest statement
R.J.B. reports grants from Eli Lilly, Roche, Pharma Consortium (AbbVie, AstraZeneca, Biogen, Eisai, Eli Lilly and Company, Hoffmann La‐Roche Inc, Janssen, Pfizer, Sanofi‐Aventis), and Tau SILK/PET Consortium (Biogen/AbbVie/Lilly); non‐financial support from Avid Radiopharmaceuticals; personal fees and other from Washington University, outside the submitted work. J.C.M. is currently participating in clinical trials of antidementia drugs from Eli Lilly and Company, Biogen, and Janssen. J.C.M. serves as a consultant for Lilly USA and receives research support from Eli Lilly/Avid Radiopharmaceuticals. T.B. receives grant funding from Avid Radiopharmaceuticals/Eli Lilly and participates in clinical trials sponsored by Eli Lilly, Avid Radiopharmaceuticals, Roche, and Pfizer. F.L. holds grants from NIH, NIA, Alzheimer Association, DIAN, Tau‐Consortium, Large PD, Biogen, and Roche. J.L. reports speaker fees from Bayer Vital, Biogen, EISAI, TEVA, Zambon, Merck, and Roche; consulting fees from Axon Neuroscience, EISAI, and Biogen; author fees from Thieme medical publishers and W. Kohlhammer GmbH medical publishers; and is an inventor in a patent “Oral Phenylbutyrate for Treatment of Human 4‐Repeat Tauopathies” (EP 23 156 122.6) filed by LMU Munich. In addition, J.L. reports compensation for serving as chief medical officer for MODAG GmbH, is beneficiary of the phantom share program of MODAG GmbH, and is an inventor in a patent “Pharmaceutical Composition and Methods of Use” (EP 22 159 408.8) filed by MODAG GmbH, all activities outside the submitted work. R.J.P.’s laboratory receives cost recovery funding from Biogen for tissue procurement and processing services related to ALS clinical trials, outside the submitted work. All other authors have declared no conflicts of interest. Author disclosures are available in the supporting information.
Figures
References
-
- Stephen R, Hongisto K, Solomon A, Lönnroos E. Physical activity and Alzheimer's disease: a systematic review. J Gerontol A Biol Sci Med Sci. 2017;72(6):733‐739. - PubMed
MeSH terms
Substances
Grants and funding
- SG-20-690363-DIAN/ALZ/Alzheimer's Association/United States
- HU21C0066/Korea Dementia Research Center
- Korea Dementia Research Center
- U19AG032438/AG/NIA NIH HHS/United States
- Canadian Institute of Health Research
- Brain Canada Foundation
- Japan Agency for Medical Research and Development
- Fonds de Recherche du Québec - Santé
- U19 AG032438/AG/NIA NIH HHS/United States
- Korea Health Industry Development Institute
- N/A/Deutsches Zentrum für Neurodegenerative Erkrankungen
- Raul Carrea Institute for Neurological Research
- Spanish Institute of Health Carlos III
- K01 AG073526/AG/NIA NIH HHS/United States
- AARFD-21-851415/ALZ/Alzheimer's Association/United States
