

Neutralizing Antibody Immune Correlates for a Recombinant Protein Vaccine in the COVAIL Trial
- PMID: 39325506
- PMCID: PMC11797383
- DOI: 10.1093/cid/ciae465
Neutralizing Antibody Immune Correlates for a Recombinant Protein Vaccine in the COVAIL Trial
Abstract
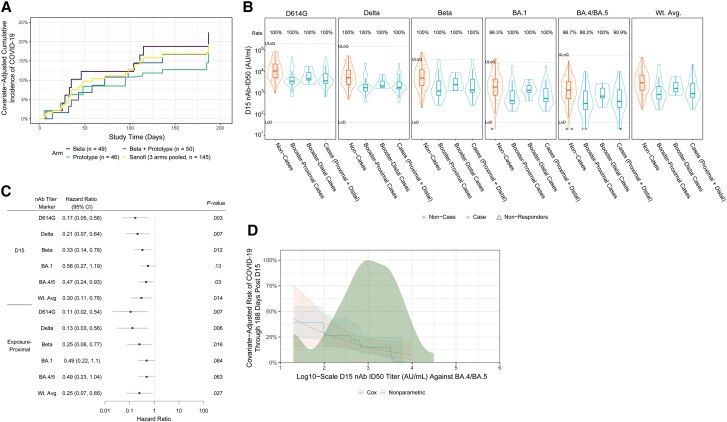
For COVAIL recipients of a coronavirus disease 2019 (COVID-19) Sanofi booster vaccine, neutralizing antibody titers were assessed as a correlate of risk (CoR) of COVID-19. Peak and exposure-proximal titers were inverse CoRs with covariate-adjusted hazard ratios (95% confidence intervals) 0.30 (0.11, 0.78) and 0.25 (0.07, 0.85) per 10-fold increase in weighted average titer.
Trial registration: ClinicalTrials.gov NCT05289037.
Keywords: COVID-19 booster; Omicron; correlate of risk; exposure-proximal titer; variant vaccine booster.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through our RightsLink service via the Permissions link on the article page on our site—for further information please contact journals.permissions@oup.com.
Conflict of interest statement
D. J. D. received an award to his institution from Leidos Biomed/NIH to conduct the clinical trial reported in the manuscript. A. R. F. reports in the past 36 months research grants to her institution from Janssen, Merck, CyanVac, VaxCo, BioFire Diagnostics, Moderna, Pfizer, and AstraZeneca; consulting fees from ADMA Biologics, GSK, Sanofi Pasteur, and Merck; support for attending meetings and/or travel from GSK, Moderna, and Sanofi Pasteur; and participation on a Novavax Data Safety Monitoring Board or Advisory Board. L. R. B received an NIH grant to his institution for the present manuscript; reports grants from NIH, Harvard Medical School, Wellcome Trust, and the Gates Foundation to his institution in the past 36 months; and participated in an NIH DSMB meeting in the past 36 months and an FDA AMDAC Committee in the past 36 months. L. R. B. is involved in human immunodeficiency virus (HIV) and SARS-CoV-2 vaccine clinical trials conducted in collaboration with the NIH, HIV Vaccine Trials Network (HVTN), COVID Vaccine Prevention Network (CoVPN), International AIDS Vaccine Initiative (IAVI), Crucell/Janssen, Moderna, Military HIV Research Program (MHRP), the Gates Foundation, and Harvard Medical School.
Figures
References
-
- Johns Hopkins Coronavirus Resource Center . Region—United States. Available at: https://coronavirus.jhu.edu/region/united-states. Accessed 12 March 2024. Last updated 10 March 2023.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- R37AI054165/National Institute of Allergy and Infectious Diseases
- 75N93021D00021/AI/NIAID NIH HHS/United States
- I01 BX000207/BX/BLRD VA/United States
- 75N93021C00012/AI/NIAID NIH HHS/United States
- UM1 AI148685/AI/NIAID NIH HHS/United States
- I01 CX002688/CX/CSRD VA/United States
- C0000008/CL/CLC NIH HHS/United States
- UM1 AI068614/AI/NIAID NIH HHS/United States
- R37 AI054165/AI/NIAID NIH HHS/United States
- UM1 AI148684/AI/NIAID NIH HHS/United States
- UM1 AI068635/AI/NIAID NIH HHS/United States
- 75N910D00024/CA/NCI NIH HHS/United States
- 75A50122C00008/Administration for Strategic Preparedness and Response
- Sanofi
- W15QKN-16-9-1002/US Department of Defense Joint Program Executive Office for Chemical, Biological, Radiological, and Nuclear Defense
- UM1AI148684/Infectious Diseases Clinical Research Consortium
- UM1 AI068618/AI/NIAID NIH HHS/United States
- UM1 AI148573/AI/NIAID NIH HHS/United States
- 75A50122C00008/Biomedical Advanced Research and Development Authority
- NH/NIH HHS/United States
- HH/HHS/United States
LinkOut - more resources
Full Text Sources
Medical
