

Targeting epigenetic regulation and post-translational modification with 5-Aza-2' deoxycytidine and SUMO E1 inhibition augments T-cell receptor therapy
- PMID: 39326886
- PMCID: PMC11425949
- DOI: 10.1136/jitc-2023-008654
Targeting epigenetic regulation and post-translational modification with 5-Aza-2' deoxycytidine and SUMO E1 inhibition augments T-cell receptor therapy
Abstract
Background: Cellular immunotherapy using modified T cells offers new avenues for cancer treatment. T-cell receptor (TCR) engineering of CD8 T cells enables these cells to recognize tumor-associated antigens and tumor-specific neoantigens. Improving TCR T-cell therapy through increased potency and in vivo persistence will be critical for clinical success.
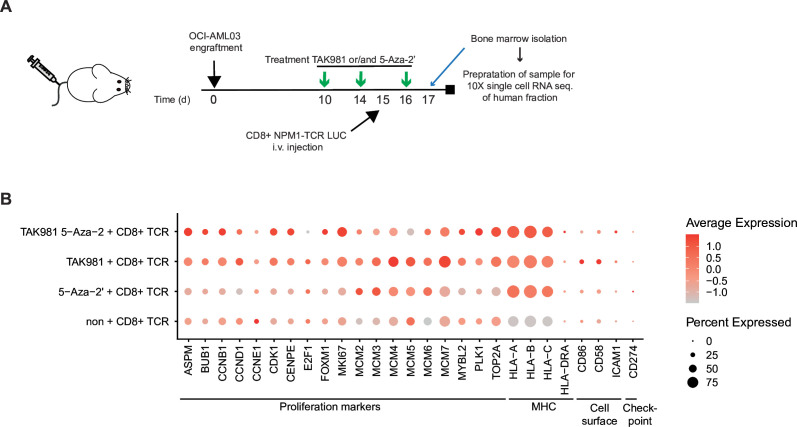
Methods: We evaluated a novel drug combination to enhance TCR therapy in mouse models for acute myeloid leukemia (AML) and multiple myeloma (MM).
Results: Combining TCR therapy with the SUMO E1 inhibitor TAK981 and the DNA methylation inhibitor 5-Aza-2' deoxycytidine resulted in strong antitumor activity in a persistent manner against two in vivo tumor models of established AML and MM. We uncovered that the drug combination caused strong T-cell proliferation, increased cytokine signaling in T cells, improved persistence of T cells, and reduced differentiation towards exhausted phenotype. Simultaneously the drug combination enhanced immunogenicity of the tumor by increasing HLA and co-stimulation and surprisingly reducing inhibitory ligand expression.
Conclusion: Combining T-cell therapy with TAK981 and 5-Aza-2' deoxycytidine may be an important step towards improved clinical outcome.
Keywords: Combination therapy; T cell; T cell Receptor - TCR.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: LUMC has applied for a patent on the triple therapy with MHMH and ACOV as inventors.
Figures






References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials