

Bending the rules: A novel approach to laryngeal surgery in a body donor study
- PMID: 39327800
- PMCID: PMC11717936
- DOI: 10.1002/hed.27939
Bending the rules: A novel approach to laryngeal surgery in a body donor study
Abstract
Background: Transoral laser microsurgery, the standard surgical approach for early-stage laryngeal cancer, necessitates an unobstructed line of sight to the operating field. However, achieving adequate laryngeal exposure can be challenging, potentially compromising treatment outcomes.
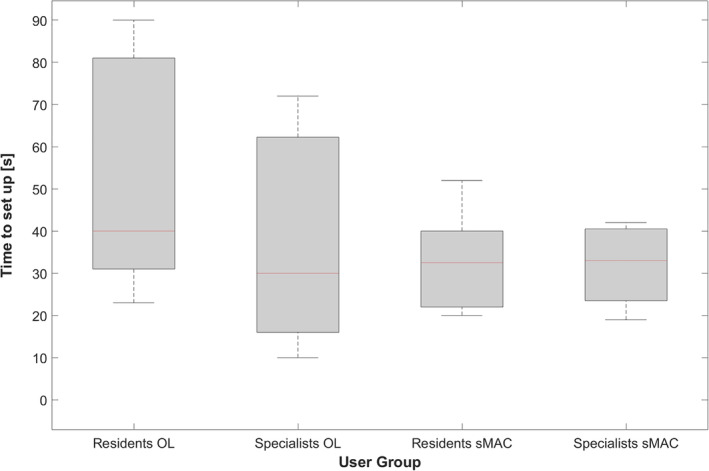
Methods: We developed a 3D-printed curved laryngoscope (sMAC), designed to match the upper airway anatomy. In a user study (n = 15) with a human body donor we compared the sMAC system to conventional microlaryngoscopy regarding laryngeal exposure and accessibility in a difficult exposure scenario.
Results: All 15 participants achieved complete glottic exposure and successfully manipulated laryngeal landmarks using the sMAC system. Only four participants achieved partial exposure using microlaryngoscopy. Positioning of the sMAC system was significantly faster (p = 0.023). A vocal cord resection was conducted successfully (n = 2) using the sMAC system.
Conclusion: The sMAC system effectively addresses challenges associated with transoral laryngeal surgery. Ongoing development aims to overcome current limitations of the system and prepare first clinical trials.
Keywords: 3D‐printing; difficult laryngeal exposure; laryngeal cancer; laryngeal surgery; transoral surgery.
© 2024 The Author(s). Head & Neck published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures





Similar articles
-
Evaluation of a curved surgical prototype in a human larynx.Eur Arch Otorhinolaryngol. 2021 Aug;278(8):2927-2935. doi: 10.1007/s00405-021-06791-9. Epub 2021 Apr 22. Eur Arch Otorhinolaryngol. 2021. PMID: 33885971 Free PMC article.
-
Preoperative clinical predictors of difficult laryngeal exposure for microlaryngoscopy: the Laryngoscore.Laryngoscope. 2014 Nov;124(11):2561-7. doi: 10.1002/lary.24803. Epub 2014 Jun 26. Laryngoscope. 2014. PMID: 24964904
-
[Applying a rigid curved video laryngoscope in laryngeal microsurgery of patients with difficult laryngeal exposure].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2022 Jun;36(6):463-466. doi: 10.13201/j.issn.2096-7993.2022.06.011. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2022. PMID: 35822366 Free PMC article. Chinese.
-
Transoral laser microsurgery for early laryngeal cancer.Expert Rev Anticancer Ther. 2010 Mar;10(3):331-8. doi: 10.1586/era.10.10. Expert Rev Anticancer Ther. 2010. PMID: 20214514 Review.
-
[Functional organ preservation in laryngeal and hypopharyngeal cancer].Laryngorhinootologie. 2011 Mar;90 Suppl 1:S83-109. doi: 10.1055/s-0030-1270449. Epub 2011 Apr 26. Laryngorhinootologie. 2011. PMID: 21523635 Review. German.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
