

Arterial spin labeling detects trapped labeled spins in flow-diverted aneurysms and it reflects intra-aneurysmal flow stasis
- PMID: 39327948
- PMCID: PMC11559746
- DOI: 10.1177/15910199241286130
Arterial spin labeling detects trapped labeled spins in flow-diverted aneurysms and it reflects intra-aneurysmal flow stasis
Abstract
Background: This study evaluated arterial spin labeling (ASL) imaging findings in flow-diverted aneurysms (FD-ANs).
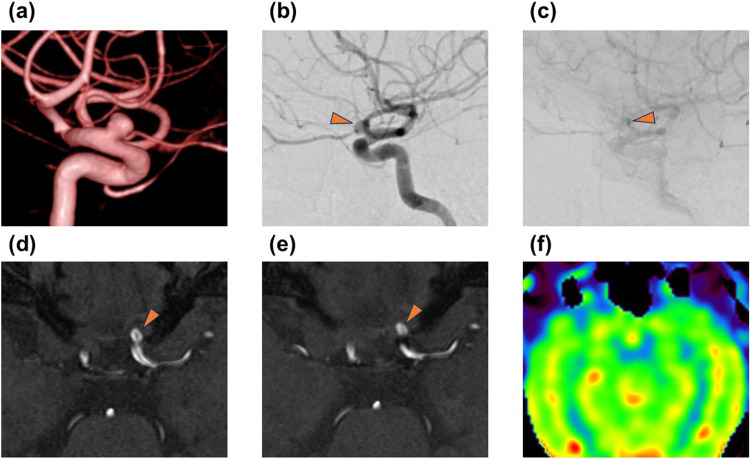
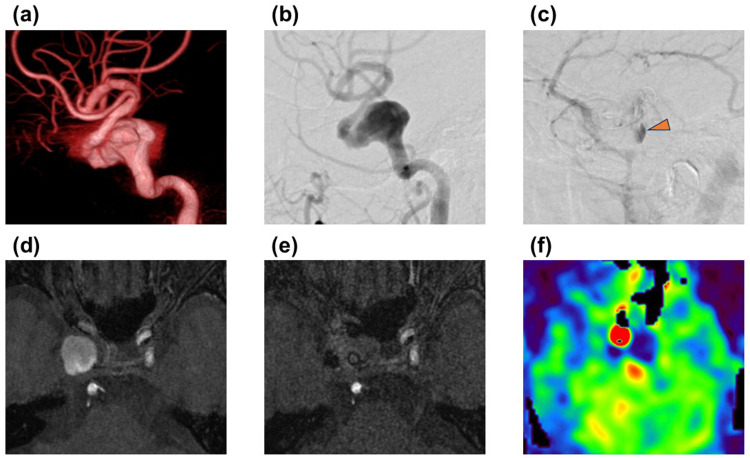
Methods: Twenty-one patients with internal carotid artery aneurysms treated with flow-diverter stent (FDS) were included. Time-of-flight magnetic resonance angiography (TOF-MRA) and ASL were performed before and after follow-up digital subtraction angiography (DSA) on the day, 6 months, and/or 1 year after treatment. Two radiologists rated the clarity of the depiction of FD-ANs for MRA on a 3-point scale and the ASL signal intensity of the aneurysm as negative or positive. A neurosurgeon assessed DSA findings using the O'Kelly-Marotta (OKM) grading scale, categorizing them into filling and stasis grades. The 23 examinations were classified according to the OKM grading scale, and the proportion of ASL-positive cases and the proportion of cases with MRA scores of 1-2 (detectable) were calculated for each grade. The relationship between the OKM grading scale and ASL positivity or MRA detectable was examined using Fisher's exact test.
Results: Of seven examinations where the statis grade was 1 or 2, no examinations showed ASL positivity. However, among the 16 examinations in which the stasis grade was 3, 9 examinations showed ASL positivity. A significant association was observed between stasis grade and ASL positivity (p = 0.035). In contrast, no significant relationship was observed between the OKM grading scale and the MRA 3-point scale.
Conclusion: High-signal ASL in FD-ANs could reflect stasis within the aneurysm; therefore, noninvasive ASL can indicate reduction in intra-aneurysmal blood flow after treatment and reperfusion during posttreatment observation.
Keywords: Aneurysm; endovascular procedures; magnetic resonance angiography; perfusion magnetic resonance imaging.
Conflict of interest statement
Declaration of conflicting interestsThe authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

Similar articles
-
"Trapped labelled spins"-related signal on arterial spin labelling in the assessment of flow-diverted aneurysms: preliminary experience.Neuroradiology. 2022 Jan;64(1):77-93. doi: 10.1007/s00234-021-02721-y. Epub 2021 Jun 14. Neuroradiology. 2022. PMID: 34128085
-
Predicting the O'Kelly-Marotta scale score after flow-diverter stent placement using silent MRA.Jpn J Radiol. 2024 Dec;42(12):1403-1412. doi: 10.1007/s11604-024-01632-1. Epub 2024 Aug 29. Jpn J Radiol. 2024. PMID: 39207642 Free PMC article.
-
Postprocedural, midterm, and long-term results of cerebral aneurysms treated with flow-diverter devices: 7-year experience at a single center.Neurosurg Focus. 2017 Jun;42(6):E3. doi: 10.3171/2017.3.FOCUS1732. Neurosurg Focus. 2017. PMID: 28565988
-
MRA versus DSA for the follow-up imaging of intracranial aneurysms treated using endovascular techniques: a meta-analysis.J Neurointerv Surg. 2019 Oct;11(10):1009-1014. doi: 10.1136/neurintsurg-2019-014936. Epub 2019 May 2. J Neurointerv Surg. 2019. PMID: 31048457 Review.
-
Intracranial 3D and 4D MR Angiography Using Arterial Spin Labeling: Technical Considerations.Magn Reson Med Sci. 2020 Dec 1;19(4):294-309. doi: 10.2463/mrms.rev.2019-0096. Epub 2019 Nov 22. Magn Reson Med Sci. 2020. PMID: 31761840 Free PMC article. Review.
References
-
- Thamburaj K, Zammar S, Tsay A, et al. Magnetic resonance angiography after flow diversion: the use of complementary magnetic resonance angiography techniques to monitor aneurysm occlusion and device and arterial branch patency after flow diverter placement. World Neurosurg 2022; 162: e147–e155. - PubMed
-
- Patzig M, Forbrig R, Ertl L, et al. Intracranial aneurysms treated by flow-diverting stents: long-term follow-up with contrast-enhanced magnetic resonance angiography. Cardiovasc Intervent Radiol 2017; 40: 1713–1722. - PubMed
LinkOut - more resources
Full Text Sources
