

Making Living-donor Liver Transplantation a Viable Option for Patients With Portopulmonary Hypertension
- PMID: 39328251
- PMCID: PMC11427031
- DOI: 10.1097/TXD.0000000000001710
Making Living-donor Liver Transplantation a Viable Option for Patients With Portopulmonary Hypertension
Abstract
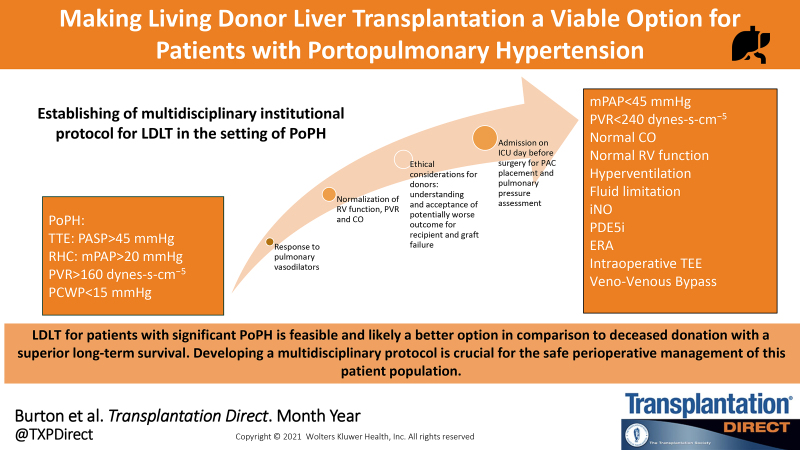
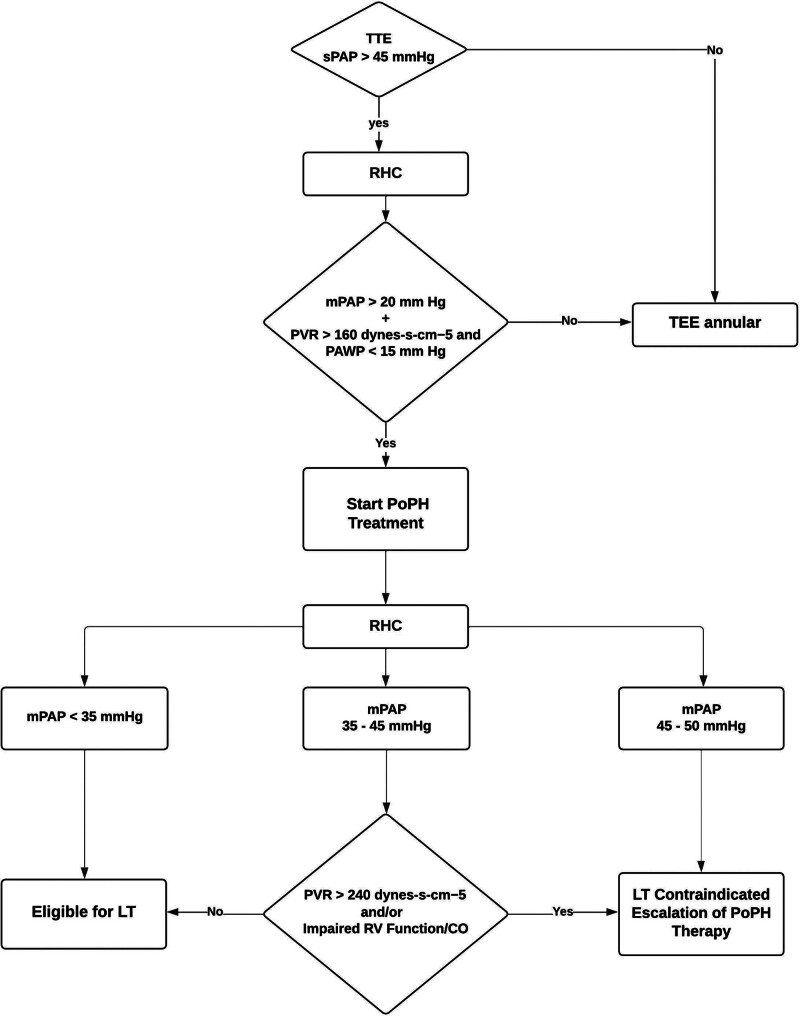
Liver transplantation (LT) in patients with significant portopulmonary hypertension (PoPH) is associated with an increased risk of several complications, including graft failure. Graft loss is one of the major reasons. Living donor LT (LDLT) is not routinely performed in the United States in this patient population. In addition, ethical considerations often preclude donation from healthy donors in the setting of a procedure associated with an elevated risk of recipient morbidity and mortality. However, LDLT allows LT to be performed electively, using a superior graft with an improved probability of a good outcome. The key to success in managing these patients is establishing a multidisciplinary team that follows an institutional protocol with clear evaluation and management criteria. These criteria include screening and early diagnosis as well as treatment of PoPH with the goal of optimizing pulmonary arterial hemodynamics and maintaining right ventricular function. Any protocol should include admitting the patient to the hospital a day before surgery for placement of a pulmonary artery catheter to measure and derive relevant hemodynamic variables. A multidisciplinary team should determine the fitness for a transplant a after a careful review of the most up-to-date clinical information. Finally, the team prescribes and executes a plan for optimization and safe perioperative management of the patient. In this report, we discuss our approach to the perioperative management of a patient with significant PoPH who safely underwent LDLT with an excellent postoperative outcome.
Copyright © 2024 The Author(s). Transplantation Direct. Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no funding or conflicts of interest.
Figures
Similar articles
-
Pulmonary Vascular Resistance Predicts Mortality and Graft Failure in Transplantation Patients With Portopulmonary Hypertension.Liver Transpl. 2021 Dec;27(12):1811-1823. doi: 10.1002/lt.26091. Epub 2021 Jun 29. Liver Transpl. 2021. PMID: 33964116 Free PMC article.
-
Portopulmonary Hypertension: Management and Liver Transplantation Evaluation.Chest. 2023 Jul;164(1):206-214. doi: 10.1016/j.chest.2023.01.009. Epub 2023 Jan 14. Chest. 2023. PMID: 36649754 Review.
-
Liver transplantation for severe portopulmonary hypertension: A case report and literature review.World J Clin Cases. 2019 Nov 6;7(21):3569-3574. doi: 10.12998/wjcc.v7.i21.3569. World J Clin Cases. 2019. PMID: 31750339 Free PMC article.
-
Comparison of Post-Liver Transplantation Outcomes in Portopulmonary Hypertension and Pulmonary Venous Hypertension: A Single-Center Experience.Transplant Proc. 2017 Mar;49(2):338-343. doi: 10.1016/j.transproceed.2016.12.006. Transplant Proc. 2017. PMID: 28219595
-
Portopulmonary hypertension.Clin Liver Dis. 2014 May;18(2):421-38. doi: 10.1016/j.cld.2014.01.004. Epub 2014 Feb 25. Clin Liver Dis. 2014. PMID: 24679504 Review.
References
-
- Simonneau G, Robbins IM, Beghetti M, et al. . Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2009;54:S43–S54. - PubMed
-
- Krowka MJ, Fallon MB, Kawut SM, et al. . International liver transplant society practice guidelines: Diagnosis and management of hepatopulmonary syndrome and portopulmonary hypertension. Transplantation. 2016;100:1440–1452. - PubMed
-
- DuBrock HM. Portopulmonary hypertension: management and liver transplantation evaluation. Chest. 2023;164:206–214. - PubMed
-
- Rodriguez-Roisin R, Krowka MJ, Herve P, et al. ; ERS Task Force Pulmonary-Hepatic Vascular Disorders (PHD) Scientific Committee. Committee ERSTFP-HVDS: pulmonary-hepatic vascular disorders (PHD). Eur Respir J. 2004;24:861–880. - PubMed
LinkOut - more resources
Full Text Sources
